Effect Head of Bed Elevation on Intra-Abdominal Pressure (IAP) in Critically Ill Patients
Made Oka Ari Kamayani
1, F. Sri Susilaningsih
2, Titin Mulyati
31Lecturer at Nursing Program, Medical Faculty, Universitas Udayana, [email protected] 2Lecturer at Nursing Faculty, Universitas Padjadjaran
3Nurse at General Intensive Care Unit (GICU) Hasan Sadikin General Hospital
ABSTRACT
Critically ill patients, which are on mechanical ventilation, present with higher intra-abdominal pressure (IAP) values when PEEP is applied and should be monitored very closely. Persistently increases IAP to 12 mmHg or greater can be affected to all body systems and the effects can lead to multisystem organ failure and death. In the intensive care unit, most ventilated patients are nursed with the head of the bed elevated (HOB) at 30° to 45° to reduce the risk of ventilator-associated pneumonia and gastric reflux. HOB elevation is limited when the patient has femoral site and hemodynamic monitoring, the bed can be raised up to 15 to 30. IAP is most commonly measured via the bladder with the patient in the supine position. Use of the supine position in patients receiving mechanical ventilation increases the risk of aspiration pneumonia developing.
A quasi-experimental of quantitative study was conducted in General Intensive Care Unit (GICU) RSUP Dr. Hasan Sadikin. A total of 23 patients on mechanical ventilation were included. Patient had IAP measured first while positioned supine without any head of bed elevation, after the patient positioned supine with HOB elevation 15 and again after the patient positioned supine with HOB elevation 30.
In the supine position, mean IAP was 11.9 ± 4.2 cmH2O. In the HOB elevation 15, mean IAP was 12.6 ± 4.4 cmH2O. In the HOB elevation 30, mean IAP was 14.5 ± 5.2 cmH2O. When analysed with post hoc pair wise comparisons, the difference of IAP between the supine position and HOB elevation 15 was not statistically significant (p>0.05), the difference of IAP between the HOB elevation 15 and HOB elevation 30 was statistically significant (p<0.05).
It is feasible to measured IAP with HOB elevation 15 and that position could be an alternative to supine positioning of patients for measurement of IAP.
Keywords: intra-abdominal pressure, HOB elevation
INTRODUCTION
Intra-Abdominal Pressure (IAP) is pressure condition on abdominal cavity. IAP on healthy people is ranged from 0-5 mmHg. Intra-Abdominal Hypertension (IAH) is the recur pathological increase of IAP more than 12 mmHg (Lee, 2012). This condition can disturb various organs such as: heart, lung, kidney gastrointestinal tract, liver and Central nervous system (Cheatam, 2009).
IAP is usually measured through bladder in which the supine position is prepared for patients (Rooban, Regli, Davis, Keulenaer, 2012). The measure of bladder pressure through an indwelling urinary catheter make up a simple and effective method for measuring IAP indirectly (Anderson, 2007). Supine position is one of aspiration risk factors due to possibility the increase of gastro-eosophageal reflex (Urden, Stacy, Lough, 2010).
the alveolous open continuously, preventing the alveolous from collapse and athelecthasis, even they don’t have other risk factors for IAH (Morejón & Barbeito, 2012). Thie increase of PEEP disturbs the expansion of the abdominal cavity (Valenza et al., 2007 dalam Jakob, Knuesel, Tenhunen, Pradl, Takala, 2010).
Strip the normal defense mechanisms, often stalled when patient prescribed for mechanical ventilation, the decreased of mobility and also impaired cough reflex can cause infection in the lungs (Smeltzer, Bare, Hinkle, Cheever, 2008). Aspiration may occur before, during, or after intubation (Hudak & Gallo, 2010). Aspiration of oropharyngeal pathogenic organisms are believed to cause pneumonia in the majority of nosocomial pneumonia (Marino, 2007). One of the measures to prevent aspiration is HOB elevation position at least 300 (Bulecheck, 2013; Urden, Stacy, Lough, 2010). The Centers for Disease Control and Prevention recommend that HOB elevation positions 30-45in mechanically ventilated patients prevent Ventilator-Associated Pneumonia (VAP) (Dillon, Munro, Grap, 2002).
Based on the description above can be seen the occurrence of a phenomenon in which the importance of HOB elevation position and also the importance of measuring the IAP. IAP measurement is done by adjusting the client in the supine position during the measurement thus increasing the risk of aspiration in patients with mechanical ventilation installed. Based on this phenomenon researchers assume IAP measurement with HOB position 15 and 30 elevation will not increase the value of IAP and also reduce the risk of aspiration than the supine position during the measurement of IAP.
METHODS: Study Design
This research is quantitative, using a pretest - posttest designs without control. In the pretest -posttest study designs data is collected both before and after the intervention, the changes can be measured by determining the change in the group (quasi-experimental) (Dharma, 2011; Polit & Beck, 2008).
Patients
The sample in this study were taken using incidental sampling technique. The sample in this study is 23 mechanically ventilated patients who were treated in GICU RSUP Dr. Hasan Sadikin Bandung. Inclusion criteria were the following: hemodynamically stable, 18-65 years old. Exclusion criteria were the following: patients with spinal cord injury, ascites, and plasma albumin levels < 2 mg / dl. The research was conducted on June 13 until July 6, 2014.
Tools and Data Collection Procedures
This study uses observation sheets made by the researchers themselves. Observation sheet consists of the data characteristics of respondents and the data results of the assessment and measurement obtained include: medical diagnosis, date of ICU admission, the measurement date IAP, mode of ventilator, the diet, the results of blood gas analysis (AGD), vital signs, CRT, saturation oxygen, and the IAP by the time patients are given the supine position and HOB elevation.
the IAP measurement in accordance with Standard Operating Procedures (SOPs) measurement of IAP in the room GICU. Measurements were made with the steps: set the zero point (zero point) by drawing a parallel line simpisis pubis to the lateral direction, then pull the axillary line median, connect the blood sets and threeway to Foley catheter patients, fill the syringe with liquid NaCl 0.9% at 35 ml, the contents manometer with liquid NaCl 0.9% to zero by turning the threeway towards manometer, cap toward the patient, turn back threeway towards patients, cap toward manometer, enter the fluid NaCl 0.9% 25 ml, cap askew wait 30-60 seconds. Readings were taken at the end of expiration.
Statistic
Comparison of IAP in the supine, HOB elevation 15, and position measurement HOB HOB elevation 15 and 30 elevation as well as the measurement of supine and HOB elevation 30 IAP categorized in a lower, fixed, and rising. Presentation of the data is arranged in a frequency distribution table using percentages. The analysis was repeated ANOVA to analyze the comparison IAP in the supine position , HOB elevation 15 and 30.
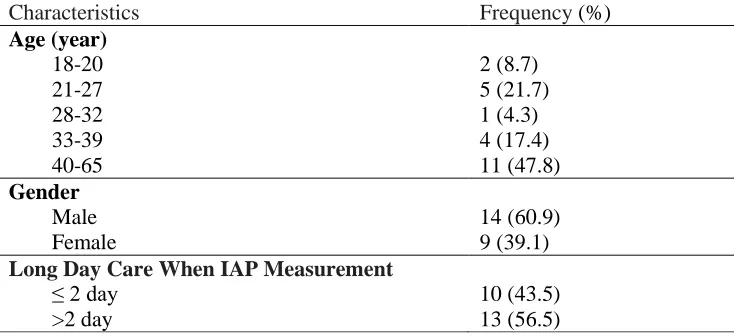
Based on Table 4.1 . it can be seen the age of the respondents are most common in the age range 40-65 years as many as 11 respondents ( 47.8 % ). By sex, the majority of respondents are male as many as 14 respondents ( 60.9 % ). The age of the respondents are most common in the age range 40-65 years as many as 11 respondents ( 47.8 % ) . By sex, the majority of respondents are male as many as 14 respondents ( 60.9 % ). Based long day care at the time of measurement GICU IAP, as many as 13 respondents ( 56.5 % ) were treated > 2 days.
Tabel 4.2. The Average Value of the measurement of IAP (Repeated Anova) Position Measurement IAP Average of IAP + SD
(in cmH2O)
p
HOB elevation 15 12.6 ± 4.4 0.01
HOB elevation 30 14.5 ± 5.2
Based on the table 4.2. can be seen the value of p 0.01 ( less than 0.05 ) means that there are differences in measurement results IAP in the supine position , HOB elevation 15 and 30. To determine the position of the different IAP measurement then performed a post hoc analysis Paired Wise Comparisons.
Tabel 4.3. Post hoc pair wise comparisons
Position Measurement IAP The average difference of IAP (dalam cmH2O, IK 95%)
Based on the table 4.3. p-value measurement can be seen IAP supination and HOB elevation 15 is 0.48 ( greater than 0.05 ) means there is no difference in the measurement results IAP in the supine position and HOB elevation 15. P-value measurement of IAP position HOB elevation 15 and HOB elevation 30 is 0.00 (less than 0.05) means that there are differences in measurement results IAP in a position HOB elevation 15 and HOB elevation 30.
DISCUSSION
The results are consistent with research Cresswell et al. (2012) LIAP value at HOB elevation 30 higher than the supine position. The results are consistent with research Rooban, Regli, Davis, Keulenaer (2012), IAP is measured using a pressure bladder is affected by the change in position from a supine position to position HOB elevation 30. There is an average increase of IAP measurement results at HOB position 30 elevation than the supine position.
Results of this study are also consistent with research McBeth et al. (2007) conducted a study to compare the results of measurements of IAP via intravesical at an angle ranging from 0-45. The result showed that the increase in IAP was significantly associated with an increased HOB elevation, significant changes occur in the position of HOB elevation> 20. Recommendations to improve the development of the abdominal wall covering to avoid the prone position and avoid positions HOB elevation of more than 20 (Lee, 2012).
Upright position gives rise to severe hydrostatic caused by abdominal organs and the body's tendency to suppress bladder (Cresswell, AB et al., 2012). Intra-abdominal pressure will rise if the volume of acute abdominal cavity increases and exceeds the capacity of its (Feliciano & Moore, 1996 in Soemarko, 2004). According, Waele, Powell, Malbrain (2009) in Rooban, Regli, Davis, Keulenaer (2012), an increase in IAP between supination and HOB elevation 30 not yet clearly known, the possibility of increasing pressure on the entire abdomen or indicates a pressure gradient in the abdomen caused by fluid flow or hydrostatic pressure on the abdominal organs due to pressure on the bladder or redistributing a localized pressure differences.
HOB position 15 elevation on an increase in the average IAP compared to the supine position, but when performed statistical tests, the average increase is not significant. This is probably due to the position 15 HOB elevation occurs contraction of the muscles of the abdomen are minimal effect on suppression muscles of the abdominal wall and bladder pressure were minimal so it does not cause a significant increase in IAP measurement results.
Pascal's Law which states that the pressure exerted on the liquid in the enclosed space is passed in all directions with equal size. This pressure is called hydrostatic pressure (hydrostatic pressure). The amount of pressure is affected by gravity (Fairman, 1996). Hydrostatic weight gain caused by the organs of the abdomen at HOB position 15 elevation is not too large so that pressure is passed into the bladder is not too big .
CONCLUSION
There was no difference in the measurement values IAP supine position and HOB HOB elevation 15. HOB elevation 15 a safe position for the measurement of IAP because it does not cause an increase in IAP measurement results. There are differences in the measurement position value IAP HOB elevation 15 and HOB elevation 30. The results of this research prove there was no difference in the value of IAP in the supine position and HOB elevation 15 so that it can be used as evidence based position measurement of IAP using HOB elevation 15 to prevent aspiration.
REFERENCES
Bulechek, G.M. et al. (2013). Nursing Intervention Classification (NIC). United Stated of America, Elsevier Inc.
Cheatam, M.L. (2009). Abdominal Compartment Syndrome: Pathophysiology and Definitions. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine, 17, 10. doi:10.1186/1757-7241-17-10.
Cheatam, M.L. et al. (2009). The Impact of Body Position on Intra-Abdominal Pressure Measurement: A Multicenter Analysis. Critical Care Medicine, 37 (7): 2187-90. doi:
10.1097/CCM.0b013e3181a021fa.
Cresswell, A.B. (2012). The Effect of Body Position on Compartmental Intra-Abdominal Pressure Following Liver Transplantation. Annals of Intensive Care, 2 (Suppl 1).
Dharma, K. K. (2011). Metodelogi Penelitian Keperawatan: Panduan Melaksanakan dan Menera pkan Hasil Penelitian. Jakarta, Trans Info Media.
Dillon, A., Munro, C.L., Grap M.J. (2002). Nurses' Accuracy in Estimating Backrest Elevation. American Journal of Critical Care, 11, 34-37.
Fairman, J.G. (1996). Pascal's Principle and Hydraulics. Melalui www.grc.nasa.gov. (21/07/2014).
Hudak C.M. & Gallo B.M. (2010). Critical Care Nursing: A Holistic Approach. Philadelphia: J.B. Lippincott Company.
Jakob, S.M., Knuesel, R., Tenhunen, J.J., Pradl, R., Takala, J. (2010). Increasing Abdominal Pressure with and without PEEP: Effects on Intra-Peritoneal, Intra-Organ and Intra-Vascular Pressures. BMC Gastroenterology, 10:70.
Lee, S.K. (2012). Intra-abdominal Hypertension and Abdominal Compartment Syndrome: A Comprehensive Overview. Critical Care Nurse, 32, 19-32. doi: 10.4037/ccn2012662.
McBeth, P.B. et al. (2007). Effect of Patient Positioning on Intra-Abdominal Pressure Monitoring. The American Journal of Surgery, 193, Issue 5 , 644-647.
Rooban, N., Regli, A., Davis, W.A., Keulenaer, B.L.D. (2012). Comparing Intra-Abdominal Pressures in Different Body Positions Via A Urinary Catheter and Nasogastric Tube: A Pilot Study. Annals of Intensive Care, 2 (Suppl 1), S11.
Smeltzer, S.C., Bare, B.G., Hinkle, J.L., Cheever, K.H. (2008). Brunner & Suddarth’s Textbook of Medical Surgical Nursing. Philadelphia, Lippincott Williams & Wilkins.
Soemarko, M. (2004). Hubungan Peningkatan Tekanan Intravesika Urinaria dengan Perdarahan Intraperitoneal akibat Trauma Tumpul Abdomen. Jurnal Kedokteran Brawijaya, 20, 25-29.
Urden, L. D., Stacy, K.M., Lough, M.E. et al. (2010). Critical Care Nursing. USA, Mosby Elsevier.