Delivered by Publishing Technology to: Aerospace Medical Association Member IP: 203.97.168.43 On: Mon, 28 Jul 2014 20:40:23
Copyright: Aerospace Medical Association
RESEARCH ARTICLE
W IRAWAN IMA, W U R, A BERNETHY M, A LDINGTON S, L ARSEN PD. Calcium scores in the risk assessment of an asymptomatic popula-tion: implications for airline pilots. Aviat Space Environ Med 2014; 85:812 – 7.
Background: This study evaluated whether coronary artery calcium score (CACS) improved cardiovascular disease risk prediction when compared to the New Zealand Cardiovascular Risk Charts (NZ-CRC), and describes the potential utilization of CACS in cardiovascular disease (CVD) risk assessment of pilots. Methods: A cross-sectional study was performed among asymptomatic patients who underwent coronary computed tomography angiography at Pacifi c Radiology Wellington, New Zealand, between August 2007 and July 2012 and had their CACS and CVD risk score calculated. Receiver-operating characteristics (ROC) analyses were used to measure the accuracy of the NZ-CRC and CACS. Reclassifi cation analyses were performed to examine the net reclassifi -cation improvement (NRI) of CACS when compared to NZ-CRC. Results: Over a 5-yr study period, 237 male asymptomatic patients with ages ranging from 30 to 69 yr with a mean (SD) of 53.24 (8.18) yr, were in-cluded. The area under the ROC curves (AUC) (95% CI) for CACS and NZ-CRC were 0.88 (0.83-0.93) and 0.66 (0.59-0.73), respectively. The NRI (95% CI) of the calcium scores was 0.39 (0.17-0.62). CACS should be assessed in pilots with 5-yr CVD risk scores of 5 – 10% and 10 – 15%.
Conclusion: CACS has a better accuracy than the NZ-CRC and reclassi-fi ed a considerable proportion of asymptomatic patients into correct car-diovascular risk categories. An approach on how the CACS should be employed in the cardiovascular risk assessment of airline pilots is noted in this paper.
Keywords: assessment tool , CACS , Framingham risk score , occupational group , risk stratifi cation .
C
ARDIOVASCULAR disease (CVD) risk stratifi ca-tion has been applied by aviaca-tion authorities in many countries. This encompasses risk prediction mod-els to generate an absolute risk of CVD over a particular time frame ( 9 ). However, previous research showed that the prediction models based on CVD risk factors are limited in their ability to discriminate between people who will or will not experience CVD ( 8 ). Our previous study found that, in spite of seemingly appropriate cut-off points, the risk assessment tool had a low sensitivity and was unable to predict almost half of CVD events. More than half (60%) of the CVD events observed oc-curred as sudden clinical presentations and almost half (47%) of the cardiovascular events occurred in pilots whose highest 5-yr CVD risk was in the 5 – 10% range ( 20 ).The New Zealand Civil Aviation Authority evaluates the cardiovascular risk of medical certifi cate applicants using New Zealand Cardiovascular Risk Charts (NZ-CRC) published by the New Zealand Guideline Group
(NZGG) ( 4 , 13 ). The NZ-CRC yields 5-yr risk estimations of , 2.5%, 2.5 – 5%, 10 – 15%, 15 – 20%, and . 20% ( Fig. 1 ); for the purpose of the CAA medical standards, a 5-yr CVD risk of 10% (approximate 10-yr CVD risk of 20%) or higher is considered excessive ( 3 ). Our previous study found that the current approach to investigate excessive cardiovascular risk in pilots, however, relies heavily on exercise electrocardiograms as a diagnostic test and may not be optimal either to detect disease or to protect pi-lots from unnecessary invasive coronary angiography. A more comprehensive and accurate cardiac investiga-tion algorithm to assess excessive CVD risk in pilots is required ( 19 ).
Previous studies have indicated that quantifi cation of coronary artery calcium score (CACS) using computed tomography (CT) is one of the methods that can improve risk prediction over conventional risk prediction models such as the Framingham Risk Score. Available guidelines, recommendations, systematic reviews, and meta-analy-ses relevant to cardiovascular risk asmeta-analy-sessment in asymp-tomatic adults demonstrated that CACS testing is the best candidate to be applied for cardiovascular risk as-sessment in people at intermediate risk or 10 – 20% over 10 yr ( 5 , 15 , 16 ). A clinical expert consensus also sup-ported that CACS has a progressively higher level of quality evidence in its role in risk stratifi cation of asymp-tomatic populations ( 7 ).
To the best of our knowledge, however, evidence that CACS improves cardiovascular disease risk prediction when compared to the NZ-CRC is still limited. This is important due to the fact that NZ-CRC has some differ-entiation from the basic Framingham risk score and other cardiovascular risk prediction tools applied by different
From the Occupational and Aviation Medicine Unit, University of Otago, Wellington, New Zealand, and the Occupational Health Department, Udayana University, Bali, Indonesia.
This manuscript was received for review in November 2013 . It was accepted for publication in April 2014 .
Address correspondence and reprint requests to: I. Made Ady Wirawan, M.D., M.P.H., Occupational Health Department, Udayana University, Jl PB Sudirman, Denpasar, Bali, Indonesia; ady.wirawan@ otago.ac.nz or [email protected] .
Reprint & Copyright © by the Aerospace Medical Association, Alexandria, VA.
DOI: 10.3357/ASEM.3904.2014
Calcium Scores in the Risk Assessment of an
Asymptomatic Population: Implications for
Airline Pilots
Delivered by Publishing Technology to: Aerospace Medical Association Member IP: 203.97.168.43 On: Mon, 28 Jul 2014 20:40:23
Copyright: Aerospace Medical Association
countries. This study aimed at proving that CACS also has a better accuracy than the NZ-CRC and more importantly examined the reclassifi cation improvement of CACS if it is used as a screening tool in comparison with the NZ-CRC. Based on the results, potential utiliza-tion of CACS in CVD risk assessment of pilots is then presented.
METHODS
Subjects
Asymptomatic patients who underwent a coronary computed tomography angiography (CCTA) at Pacifi c Radiology Wellington, New Zealand, were included in this study. The main inclusion criteria were patients, ages between 30-70 yr old, who were referred for cardio-vascular risk assessment and cardiac investigation. The
exclusion criteria included: reasons for referral were un-available; cardiovascular risk score could not be calcu-lated; or coronary artery calcium scores were unavailable. Patients with established cardiovascular diseases or who had experienced one or more previous CVD events, percutaneous coronary intervention, or coronary artery bypass graft surgery, were also excluded from this study.
Procedure
This was an observational, cross-sectional diagnostic accuracy study using data collected between 1 August 2007 and 26 July 2012. The main variables tested were CVD risk score and CACS. The 5-yr risk of a cardiovas-cular event was calculated using the NZ-CRC ( 13 ) based on CVD risk factors, including: age, gender, systolic blood pressure, smoking history, diabetes status, and total cholesterol-HDL ratio. Risk scores are classifi ed as:
Delivered by Publishing Technology to: Aerospace Medical Association Member IP: 203.97.168.43 On: Mon, 28 Jul 2014 20:40:23
Copyright: Aerospace Medical Association
, 2.5%, 2.5 – 5%, 5 – 10%, 10 – 15%, 15 – 20%, 20 – 25%, 25 – 30%, and . 30%. The CVD risk factors data were retrieved from the CT Cardiac Patient Health Questionnaire fi lled out during the CT coronary angiography examination.
The technical details used for the CT coronary angiog-raphy are described as follows. Scans were performed on a GE 64-slice Discovery VCT and, since January 2011, the GE 750HD (GE Healthcare, Little Chalfont, Bucking-hamshire, UK). Patients were beta blocked with 50 or 100 mg metoprolol SR 1 h prior. All scans were ECG gated. Contrast was not given for the calcium scoring (SmartScore, GE Medical Systems, Waukesha, WI), but between 80 – 100 ml of Omnique 350 for the contrast car-diac angiogram (SnapShot Pulse, GE Healthcare) was used. Patients were given sublingual glyceryl trinitrate spray immediately prior to the contrast run unless there was a contraindication. Technical settings were very similar for both machines. For the calcium scoring the parameters were: Cine mode, 2.5 mm slice, 40 mm de-tector size, 0.35 rotation time, 120 kV tube voltage, and 200-300 mA tube current; for the cardiac angiogram (prospective acquisition), the settings were Cine high resolution mode, 0.625mm slice, 35 rotation time, 100-120 kV tube voltage, and 500-700 mA tube current. The algorithm was HD Soft. Agatston scores were calculated and classifi ed as: 0, 1-9, 10-99, 100-399, 400-999, and ⱖ 1000 for the analysis in this study. For the presence of a coronary artery disease, a stenosis of 50% or more was considered a signifi cant cardiovascular disease.
Receiver operating characteristics (ROC) analyses were used to assess the accuracy of the CVD risk score and CACS. Reclassifi cation analyses were then per-formed to examine the net reclassifi cation improvement (NRI) of CACS when it is used as a screening tool com-pared to CVD risk score. For the purpose of the reclas-sifi cation analysis, “ low risk ” is defi ned as having a
Statistical analyses were performed using R version 2.15.3 (R: a language and environment for statistical com-puting. R Foundation for Statistical Computing, Vienna, Austria). “ PredictABEL ” R package was employed for ROC and reclassifi cation analyses ( 10 ). This is a low-risk observational study based on clinically obtained data, with no intervention other than recording, classifying, counting, and analyzing of the data. This study was ap-proved by the University of Otago Ethical Committee (Human Ethics Application: Category B)
RESULTS
There were 260 asymptomatic male patients who underwent a CCTA from 1 August 2007 to 26 July 2012 at Pacific Radiology Wellington. Of these, 23 were excluded; 6 due to no calcium score, 14 with no cardio-vascular risk score, 1 with an unsatisfactory study due
to rapid heart rate, and 2 with age more than 70 yr old. The study included 237 male asymptomatic patients with ages between 30 and 70 yr old.
Table I shows the characteristics of patients undergo-ing CCTA at Pacifi c Radiology Wellundergo-ington. The patients’ ages ranged from 30 to 69 yr old with a mean (SD) of 53.24 (8.18) yr and 77% were in the 35-60 yr category. The CVD risk calculation showed that the number of patients with 5-yr CVD risk scores of , 5%, 5 – 10%, and . 10% were 55 (23%), 87 (37%), and 95 (40%), respectively.
Coronary artery calcium (Agatston) scores of the pa-tients ranged from 0 to 1781, with a mean (SD) of 140 (292) and median (interquartile range) of 11 (142). There were 20 (8.44%) of them who had calcium scores rang-ing from 400-999 and 6 (2.53%) patients who had calcium scores of ⱖ 1000. Stenosis grading on CCTA indicated that 52 (22%) patients had a stenosis of 50% or higher (signifi cant disease) and 185 (78%) patients had a steno-sis of , 50%.
The reasoning for undergoing cardiac investigation in the asymptomatic patients is described in Table II . This table indicates that the majority of patients were referred due to having a family history of premature ischemic heart disease alone or in combination with the presence of one or more cardiovascular risk factors such as hyper-tension, hyperlipidemia, diabetes, or having an elevated cardiovascular risk. Approximately 24% of the patients underwent investigation for screening or general medi-cal check purposes. Similar fi ndings were found be-tween patients with stenosis of or more than 50% and those with stenosis less than 50%. Furthermore, six of
TABLE I. CHARACTERISTICS OF ASYMPTOMATIC PATIENTS WHO UNDERWENT CCTA.
Sample Characteristics Frequency (%)
Delivered by Publishing Technology to: Aerospace Medical Association Member IP: 203.97.168.43 On: Mon, 28 Jul 2014 20:40:23
Copyright: Aerospace Medical Association
the eight patients with quite signifi cant disease (stenosis of ⱖ 70%) were referred for cardiac investigation due to having a family history of premature ischemic heart disease alone or in combination with the presence of one or more of cardiovascular risk factors or an elevated cardiovascular risk. The two others underwent CCTA because of having one or more cardiovascular risk factors.
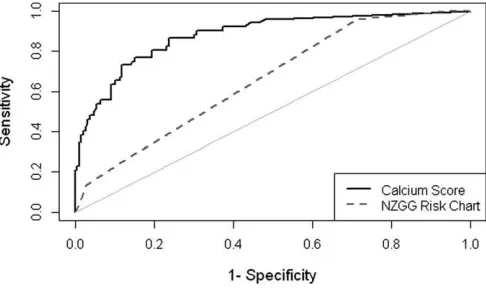
The accuracy of the NZGG risk charts and CACS in predicting cardiovascular disease is shown by Fig. 2 . The area under the ROC curve or AUC (95% CI) for CACS and the NZGG risk charts were 0.881 (0.829-0.933) and 0.661 (0.587-0.734), respectively. Reclassifi cation analysis for calcium score, when it was used as a substi-tute for the NZGG ’ s cardiovascular chart in determin-ing cardiovascular risks, includdetermin-ing NRI, is presented in
Table III . The NRI (95% CI) of the calcium scores was 0.39 (0.17-0.62), with a P -value of , 0.001.
DISCUSSION
The difference in the AUC between CACS and CVD risk score is 0.22. This clearly indicates that CACS is a better tool in predicting the presence of a coronary ste-nosis of greater than 50%. In addition, the NRI shows that calcium score correctly reclassifi ed 39% of asymp-tomatic patients into low, intermediate, and high risk categories.
The accuracy of CACS was shown in a recent systematic review on the added value of CACS in risk stratifi -cation for cardiovascular events. This review found that an increase in AUC was shown by all studies when CACS was added to the risk model, ranging from 0.05 to 0.20 ( 15 ). Other studies also found that CACS reclassi-fi ed a signireclassi-fi cant proportion of people into correct risk categories. This was shown by a NRI that ranged from 14 to 30%, where the most obvious improvement was found in those at intermediate (10 – 20% over 10 yr) Framingham risk ( 15 ). It was also estimated from the Multi-Ethnic Study of Atherosclerosis that addition of CACS measurement to the traditional risk factors model resulted in NRI in the total population of 25%, with NRI in intermediate risk individuals of about 55% and an In-tegrated Discrimination Improvement of 0.026 ( 16 ). The higher result found in our study is mainly due to the dif-ference in the risk prediction tool used and the direct comparison between NZ-CRC and CACS instead of adding CACS to the existing risk prediction model. Ad-ditionally, both NZ-CRC and CACS were assessed in a high prevalence population. In the present study, the TABLE II. RATIONALE FOR CARDIAC INVESTIGATION.
Risk Factors
Frequency (%) *
Patients with ⱖ 50% Stenosis Patients with , 50% Stenosis All Patients
FH-PIHD 16 (30.8) 63 (34.1) 79 (33.3) FH-PIHD and 1 of HT/HL/DM 10 (19.2) 33 (17.8) 43 (18.1) FH-PIHD and ⱖ 2 of HT/HL/DM 5 (9.6) 12 (6.5) 17 (7.2) FH-PIHD and elevated CV risk 1 (1.9) 1 (0.5) 2 (0.8) One of HT/HL/DM 5 (9.6) 24 (13.0) 29 (12.2) 2 or more of HT/HL/DM 2 (3.8) 5 (2.7) 7 (3.0) Elevated CV risk 1 (1.9) 3 (1.6) 4 (1.7) Screening/ Medical check-up 12 (23.1) 44 (23.8) 56 (23.6) Total 52 (100.0) 185 (100.0) 237 (100.0) * Results are presented as frequency and proportion within column.
FH-PIHD: family history of premature ischemic heart disease; HT: hypertension; HL: hyperlipidemia; DM: diabetes mellitus; CV: cardiovascular.
Fig. 2. Receiver operating characteristics of the New Zealand Cardio-vascular Risk Chart and calcium score.
TABLE III. RECLASSIFICATION TABLE FOR NZ CARDIOVASCULAR RISK CHART AND CALCIUM SCORE.
NZGG CVD Risk Score
Calcium Score
% Reclassifi ed Low Intermediate High
Patient without CVD
Low 50 3 0 6 Intermediate 53 11 1 83 High 51 12 4 94 Patient with CVD
Low 1 1 0 50 Intermediate 5 10 7 55 High 6 8 14 50 Combined Data
Low 51 4 0 7 Intermediate 58 21 8 76 High 57 20 18 81 Net reclassifi cation improvement (categorical) [95% CI]: 0.3939 [0.1662 - 0.6215]; P -value: 7e-04.
Delivered by Publishing Technology to: Aerospace Medical Association Member IP: 203.97.168.43 On: Mon, 28 Jul 2014 20:40:23
Copyright: Aerospace Medical Association
prevalence of patients with a stenosis of ⱖ 50% on CCTA was 22%. Several studies have reported results that indi-cate that diagnostic test accuracies may vary with dis-ease prevalence ( 11 ).
This suggests that the evaluation of coronary calcium is useful in primary prevention, especially in subjects classifi ed as intermediate risk based on traditional risk factors. High calcium scores identify subjects at high risk who will benefi t from aggressive prevention ap-proaches. Ferket et al. ( 5 ), who conducted a systematic review of guidelines on imaging of asymptomatic coro-nary artery disease, supported this conclusion. They found that the majority guidelines (10/14) considered CACS a test for improvement of total coronary risk as-sessment based on traditional risk factors.
This was a cross-sectional study in asymptomatic pa-tients who underwent CCTA and also had their CT cal-cium score and CVD risk score calculated. CCTA was used as the primary endpoint. While CCTA has consis-tently shown high sensitivities and specifi cities in the majority of the previous studies ( 2 ), the use of CCTA re-sults as the outcome variable and a stenosis of ⱖ 50% as the cut-off point for the presence of CVD might overes-timate the real cardiovascular events and infl uence the strength of the study. The American Society of Aerospace Medicine Specialists ( 1 ) defi ned clinically signifi -cant coronary artery disease as one or more lesions with . 50% stenosis by coronary angiography. However, the cardiovascular event rates encountered by patients with a stenosis of . 50% in the clinical population may not ac-curately predict prognosis in the younger and relatively healthier aviator population with asymptomatic disease. Another limitation of this study is that the patients were not pilots or an occupationally matched group. However, they were men and resembled the age of the commercial pilot group within New Zealand ( 17 ). De-spite all the above limitations in this study, however, the result furthers our understanding on how calcium scores can be used to improve the New Zealand cardio-vascular risk chart in the risk assessment of cardiovas-cular diseases in a group of asymptomatic individuals of similar characteristics to the pilot population.
Implications for Aviation Medicine Practices
Using calcium score as the only routine screening tool for all asymptomatic patients is not recommended ( 6 ); therefore, adding or combining calcium score into a new risk assessment approach is a reasonable way to im-prove current cardiovascular risk screening in airline pilots. Based on the results of this study and other avail-able evidence, a new system for cardiovascular investi-gation in pilot populations can be proposed.
The present CVD risk assessment states that pilots exceeding a threshold of 10% (5-yr risk) are required to demonstrate normal myocardial perfusion, generally by undergoing an exercise stress test. The pilot will be considered for further investigation, commonly through an invasive coronary angiography, if the functional test is inconclusive or positive ( 3 , 4 ). Our previous study
described how the current risk assessment has worked and concluded that the current approach to investigate excessive cardiovascular risk in pilots relies heavily on exercise electrocardiograms as a diagnostic test, and may not be optimal either to detect disease or to protect pilots from unnecessary invasive procedures ( 19 ).
A new approach in CVD risk assessment of pilots should be focused on the application of CACS in those with 5-yr CVD risk of 5 – 10% and 10 – 15% according to the New Zealand cardiovascular risk charts. A stress myocardial perfusion imaging (MPI) or coronary CT an-giography can be proposed to further investigate pilots with a calcium score of 400 or greater. The Guideline for Assessment of Cardiovascular Risk in Asymptomatic Adults ( 6 ) states that the stress MPI may be considered for advanced cardiovascular risk assessment in asymp-tomatic adults when previous risk assessment testing suggests high risk of coronary heart disease, such as a CAC score of 400 or greater. In an asymptomatic popu-lation that requires a high standard of fi tness, such as airline pilots, the utilization of stress MPI or CCTA to exclude a signifi cant coronary heart disease is reason-able before treatment or lifestyle modifi cations are initi-ated. This is practical due to the high negative predictive values of the stress MPI and CCTA.
Another consideration for using stress MPI is that this test can indicate functional myocardial perfusion. Given the fact that coronary artery calcium scoring does not provide functional evidence of obstruction, the combi-nation of CACS and stress MPI can be an ideal approach. The combination of an anatomic approach using CT cal-cium score followed by a functional approach using stress MPI will be able to identify pilots who may most benefi t from invasive coronary angiography and coro-nary revascularization.
Current evidence shows that management changes can happen after screening using a calcium score in community-based cohorts, showing that the presence of coronary calcifi cation was associated with an indepen-dent threefold greater likelihood of statin and aspirin usage ( 6 , 18 ). Data from the Multi-Ethnic Study of Atherosclerosis study also suggest that CACS . 400 was associated with a higher likelihood of initiation and con-tinuation of preventive medications ( 12 ). Furthermore, coronary artery calcium visualization is useful in moti-vating patients and increasing interactions with a health-care provider to support adherence to the lifestyle and treatment recommendations ( 6 , 14 ).
Delivered by Publishing Technology to: Aerospace Medical Association Member IP: 203.97.168.43 On: Mon, 28 Jul 2014 20:40:23
Copyright: Aerospace Medical Association
risk assessment in a specifi c occupational group such as airline pilots.
ACKNOWLEDGMENT
Authors and affi liations: I. Made Ady Wirawan, M.D., M.P.H., Occupational Health Department, Udayana University, Bali, Indonesia; Rodney Wu, M.B., Ch.B., Pacifi c Radiology Group, Wellington, New Zealand; Malcolm Abernethy, M.B., Ch.B., Wakefi eld Heart Center, Wakefi eld Hospital, Wellington, New Zealand; and I. Made Ady Wirawan, M.D., M.P.H., Sarah Aldington, M.Av.Med., Ph.D., and Peter D. Larsen, B.Sc.(Hons.), Ph.D., Occupational and Aviation Medicine Unit, University of Otago Wellington, Wellington, New Zealand.
REFERENCES
1. American Society of Aerospace Medicine Specialists . Clinical Practice Guideline for Coronary Artery Disease: developed for the Aerospace Medical Association [Internet]. ASAMS; 2007; updated 2007 April 23. Retrieved 2013 December 15 from: http://www.asams.org/guidelines/Completed/NEW%20 Coronary%20Artery%20Disease.htm .
2. Bluemke DA, Achenbach S, Budoff M, Gerber TC, Gersh B, et al. Non invasive coronary artery imaging: magnetic resonance angi-ography and multidetector computed tomangi-ography angiangi-ography: a scientifi c statement from the American Heart Association Committee on Cardiovascular Imaging and Intervention of the Council on Cardiovascular Radiology and Intervention, and the Councils on Clinical Cardiology and Cardiovascular Disease in the Young . Circulation 2008 ; 118 : 586 – 606 .
3. Civil Aviation Authority of New Zealand . Civil aviation (examina-tion procedures) general direc(examina-tions, notice 2009. Wellington, New Zealand: CAA of New Zealand; 2009 .
4. Civil Aviation Authority of New Zealand . CAA medical information sheet: cardiovascular risk. Wellington, New Zealand: CAA of New Zealand; 2010 .
5. Ferket BS, Genders TSS, Colkesen EB, Visser JJ, Spronk S, et al. Systematic review of guidelines on imaging of asymptomatic coronary artery disease . J Am Coll Cardiol 2011 ; 57 : 1591 – 600 . 6. Greenland P, Alpert JS, Beller GA, Benjamin EJ, Budoff MJ, et al.
2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and Society for Cardiovascular Magnetic Resonance . J Am Coll Cardiol 2010 ; 56 : e50 – 103 .
7. Greenland P, Bonow RO, Brundage BH, Budoff MJ, Eisenberg MJ, et al. ACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: a report of the American College of Cardiology Foundation Clinical Expert Consensus Task
Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography) developed in collaboration with the Society of Atherosclerosis Imaging and Prevention and the Society of Cardiovascular Computed Tomography . J Am Coll Cardiol 2007 ; 49 : 378 – 402 .
8. Greenland P, LaBree L, Azen SP, Doherty TM, Detrano RC . Coronary artery calcium score combined with Framingham Score for risk prediction in asymptomatic individuals . JAMA 2004 ; 291 : 210 – 5 .
9. Houston S, Mitchell S, Evans S . Application of a cardiovascular disease risk prediction model among commercial pilots . Aviat Space Environ Med 2010 ; 81 : 768 – 73 .
10. Kundu S, Aulchenko Y, Duijn C, Janssens ACW . PredictABEL: an R package for the assessment of risk prediction models . Eur J Epidemiol 2011 ; 26 : 261 – 4 .
11. Leefl ang MMG, Bossuyt PMM, Irwig L . Diagnostic test accuracy may vary with prevalence: implications for evidence-based diagnosis . J Clin Epidemiol 2009 ; 62 : 5 – 12 .
12. Nasir K, McClelland RL, Blumenthal RS, Goff DC, Hoffmann U, et al. Coronary artery calcium in relation to initiation and continuation of cardiovascular preventive medications: the Multi-Ethnic Study of Atherosclerosis (MESA) . Circ Cardiovasc Qual Outcomes 2010 ; 3 : 228 – 35 .
13. New Zealand Guideline Group . New Zealand cardiovascular guidelines handbook: a summary resource for primary care practitioners, 2nd ed. Wellington, New Zealand: New Zealand Guideline Group; 2009 .
14. O’Malley PG, Feuerstein IM, Taylor AJ . Impact of electron beam tomography, with or without case management, on motivation, behavioral change, and cardiovascular risk profi le: a randomized controlled trial . JAMA 2003 ; 289 : 2215 – 23 . 15. Peters SA, Bakker M, den Ruijter HM, Bots ML . Added value
of CAC in risk stratifi cation for cardiovascular events: a systematic review . Eur J Clin Invest 2012 ; 42 : 110 – 6 .
16. Peters SAE, den Ruijter HM, Bots ML, Moons KGM . Improve-ments in risk stratifi cation for the occurrence of cardiovascular disease by imaging subclinical atherosclerosis: a systematic review . Heart 2012 ; 98 : 177 – 84 .
17. Sykes AJ, Larsen PD, Griffi ths RF, Aldington S . A study of airline pilot morbidity . Aviat Space Environ Med 2012 ; 83 : 1001 – 5 . 18. Taylor AJ, Bindeman J, Feuerstein I, Le T, Bauer K, et al.
Community-based provision of statin and aspirin after the detection of coronary artery calcium within a community-based screening cohort . J Am Coll Cardiol 2008 ; 51 : 1337 – 41 . 19. Wirawan IMA, Aldington S, Griffi ths RF, Ellis CJ, Larsen PD .