Corresponding author: Henry Mandalas, Department of Microbiology Faculty of Dentistry Maranatha Christian Univ, Indonesia Jl. Prof.drg.Surya Sumantri No. 65, Bandung, Jawa Barat 40164. Email: [email protected]
P-ISSN 1979-0201, e-ISSN 2549-6212 Available from:http://jurnal.unpad.ac.id/pjd/index DOI:
Submission: Jun 2017 Publishing: Nov 2017
Anti-inlammatory properties of mangosteen peel extract on
the mouse gingival inlammation healing process
Khairani Putri*, Lusiana Darsono*, Henry Mandalas**
*Department of Microbiology Faculty of Dentistry Maranatha Christian University, Indonesia **Department of Periodontics Faculty of Dentistry Maranatha Christian University, Indonesia
ABSTRACT
Introduction: Mangosteen (Garcinia Mangostana L.) peel extract has widely used in the pharmaceutical
ield due to its anticancer, anti-inlammatory, antibacterial, and immunity boost properties. In the ield of dentistry, mangosteen peel extract has proofed to be able to reduce the amount of plaque, prevents plaque accumulation, and cure gingivitis. This study was aimed to determine the efect and diferences of the mangosteen peel extract at the concentration of 12.5% and 25% on the mouse gingival inlam-mation healing process. Methods: This study was a true experimental laboratory study with completely randomized design. The subjects consisted of as much as 28 mice divided into 4 groups, which were negative control (Aquadest) group; positive control (0,2% of Chlorhexidine) group; 12,5% of mangosteen peel extract group; and 25% of mangosteen peel extract group. Each group consisted of 7 mice. Exam-ination of inlammatory healing results was observed every 2 hours during 6 hours and the inlammatory measurements of mouse gingival were performed by using callipers. Data obtained was analysed with the one-way ANOVA test (α = 0,05) and the Tukey’s range test. Results: The results from the one-way ANOVA test (α = 0,05) and the Tukey’s range test found that there was a signiicant diference on the in-lammation size between the group with 12.5% of mangosteen peel extract and the group with aquadest and 0.2% of chlorhexidine. Meanwhile, the mice group with 12.5% of mangosteen peel extract and group with 25% of mangosteen peel extract did not show a signiicant diference in inlammatory size decrease. Conclusion: The mangosteen peel extract at the concentration of 12.5% and 25% were efectively used in accelerating the inlammatory healing process of the mouse gingival due to its strong anti-inlammatory efect.
INTRODUCTION
Gingivitis periodontitis is an inlammation that often occurs in the ield of dentistry. Gingivitis is included in periodontal disease. Inlammation of the gingiva or gingivitis is an inlammation that occurs in the gingiva as a result of bacterial infection. Gingivitis is characterized by changes in shape, colour, texture, and pain in the gingiva. Gingivitis usually results from poor oral hygiene.1-3
Gingivitis in Indonesia ranks second, reaching 96.58%. The Association of Indonesian Dentists (PDGI) states that the prevalence of gingivitis worldwide is 75-90%.4,5 Basic Health Research
(RISKESDAS) in 2007 mentioned that periodontal disease in West Java was the ifth largest, 25.3%.5
Clinical signs are often complained by patients who have gingivitis is easily bleed gingiva. Bleeding in the gingiva can be caused by various things. Plaque
and calculus attached to the tooth surface is the
most common cause. This cause if not treated immediately will cause the gingival attachment to
the tooth surface dislodged and form a sac on the
gum (periodontal pocket) and also cause damage to the tooth support bone.6
One way to overcome the inlammation of the gingiva is the use of herbal plant extracts. Herbal plants used as a traditional treatment ingredient one of them is the skin of mangosteen (Garcinia Mangostana L.) because this fruit contains xanthone compounds. Xanthone compounds are compounds that contain alpha-mangostin and gamma-mangostin which are as antibacterial and anti-inlammatory. Xanthone compounds play a role in the cessation of inlammation by inhibiting the production of COX enzymes that can cause inlammation.2
The results of Avira’s research in 2013 stated
that mangosteen peel extract contains xanthone
and xanthone compounds proved to have anti-inlammatory activity and very high antioxidant activity. The pathogenesis of inlammation occurs due to an increase in inlammatory cells that play
a role in the process of phagocytosis and stimulate
free radical expenditure. Antiinlammation and antioxidants play a role in converting active free radicals to less reactive and shortening the inlammatory stage to the healing stage.7
Ni Wayan Arini et al’s study on the efectiveness
of gum rinse of mangosteen peel decoction states
that the concentration of 12.5% mangosteen peel decoction decreases the amount of plaque on tooth surface, prevents plaque accumulation, and cures mild gingivitis.8 Chlorhexidine 0.2% a comparator containing 0.2% chlorhexidine gluconate, proved to be an antiplaque that can treat gingivitis and prevent periodontal abnormalities. Inlammatory measurements were performed at 2, 4, and 6 hours because the induction of carrageenan can cause
oedema that can last for six hours and gradually
diminish within 24 hours.9 The above description
leads to the need for research on the Efect of
Garcinia Mangostana L extract on the healing
process of mice gingival inlammation.
METHODS
This research is a true experimental laboratory with complete randomized design (Completely Randomized Design) so that this research is analyzed by using one-way ANOVA method followed by Tukey HSD. Animal try irst adapted for 7 days in Pharmacology Laboratory, Faculty of Medicine, Padjadjaran University, Hasan Sadikin Hospital, Bandung.
Twenty-eight Wistar rats were grouped randomly into 4 treatment groups and each group consisted of 7 tails. First anaesthesia is performed using a ketamine injected with a dose of 0.3 ml in the rat’s thighs. After the rat was anaesthetized, 0.1% of carrageenan 0.5 ml was injected in rat gingiva to form inlammation and waited for 3 h for maximum inlammation. Mice that had been divided into each group were treated in each group. Group I was applied with Aquades on inlamed gingiva, Group II was applied Chlorhexidine 0.2% in inlamed gingiva, Group III was applied with
mangosteen leaf extract (Garcinia mangostana
L.) with concentration 12,5% in inlamed gingiva, and group IV was applied mangosteen peel extract (Garcinia mangostana L.) with 25% concentration in inlamed gingiva. The measured data were the longest diameter inlammatory diameter in mm in all four groups by using the sliding term at 2, 4, and 6 hours.
RESULTS
The results of the inlammation measurement
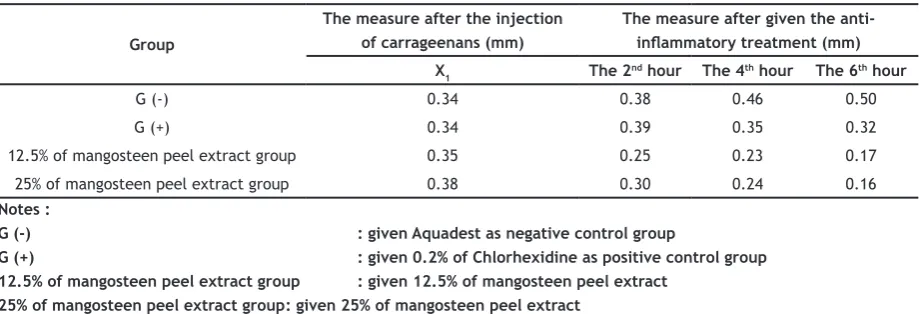
Table 1. The average of the inlammation measure of each group per hour
Group
The measure after the injection of carrageenans (mm)
The measure after given the anti-inlammatory treatment (mm)
X1 The 2nd hour The 4th hour The 6th hour
G (-) 0.34 0.38 0.46 0.50
G (+) 0.34 0.39 0.35 0.32
12.5% of mangosteen peel extract group 0.35 0.25 0.23 0.17
25% of mangosteen peel extract group 0.38 0.30 0.24 0.16
Notes :
G (-) : given Aquadest as negative control group
G (+) : given 0.2% of Chlorhexidine as positive control group 12.5% of mangosteen peel extract group : given 12.5% of mangosteen peel extract
25% of mangosteen peel extract group : given 25% of mangosteen peel extract
Figure 1 showed the mean time of decreasing
the size of gingival inlammation in the increasingly
small rats in each treatment group calculated
in hours. Diagram 1 shows the occurrence of a very rapid healing process between groups of mice given mangosteen peel extract (Garcinia Mangostana L.) 12,5% and group of mice given mangosteen skin extract (Garcinia Mangostana L.) 25%, while the negative control group aquadest with a positive control of 0.2% chlorhexidine did not show a signiicant healing process.
Before the data were analyzed using ANOVA one way, the data was irst tested by homogeneity test of variance. Obtained result 0.415 which means non-signiicant data, so it can be continued by using ANOVA one way test. Data of inlammatory
size of each group as referred to in Table 1 shows
that there is a signiicant decrease in inlammatory size at 2 o’clock so the analysis is performed. The data obtained were then analyzed statistically
Figure 1. The average of the inlammation measure of each treatment group
using ANOVA one way test with a signiicance level α = 0,05 with the hypothesis that is Ho: No efect of giving mangosteen skin extract on inlammatory size in all treatment groups. H1: There is an efect of giving mangosteen skin extract on inlammatory size to at least one pair of treatment groups. The results of statistical analysis give the following results.
Table 2 showed p-value = 0.000 <0.05 which means that there is a very signiicant diference at
least in a pair of treatment groups so that there
is a diference in inlammatory size. To ind out which group is diferent is done post hoc test by using Tukey’s range test which results as in Table 3.
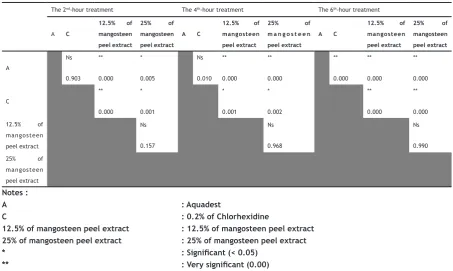
The result of statistical analysis at the 2nd hour by performing ANOVA one way test in Table 3 shows that p-value = 0,00 with α = 0,05 indicating
that there is at least one pair of treatment group
was a diference of inlammatory healing process on mouse gingiva which was signiicant (p <0,05). Diferences were found in the negative control group given aquadest and 12.5% of the mangosteen peel group (Garcinia Mangostana L.) which had the potential to decrease inlammation in rat gingiva, while aquadest with 0.2% chlorhexidine and mangosteen skin extract (Garcinia Mangostana L.) 25% there is a speed diference in the decrease of inlammation in rat gingiva.
The result of statistic analysis at the 4th hour by doing ANOVA one way test in Table 3 shows that p-value = 0,00 with α = 0,05 indicating that
there is at least one pair of treatment group that
is very meaningful. Based on statistical analysis with Tukey HSD statistic test with α = 0,05, the diference of inlammatory healing process in the gingival rat was signiicant (p <0,05). Diferences were found in the negative control group given
aquadest and groups of mice given mangosteen peel extract (Garcinia Mangostana L.) 12.5% and 25% mangosteen leather mangosteen extract (Garcinia Mangostana L.) which had the potential to decrease inlammation in rat gingiva, whereas aquadest with chlorhexidine 0.2% there was no signiicant diference in the decrease of inlammation in rat gingiva.
The result of statistical analysis at the 6th hour by doing ANOVA one way test in Table 3 shows that p-value = 0,00 with α = 0,05 indicating that
there is at least one pair of treatment group that is
very meaningful. Based on statistical analysis with Tukey HSD statistic test with α = 0,05, the diference of inlammatory healing process in the gingival rat was signiicant (p <0,05). Diferences were found in the negative control group given aquadest compared with the group given chlorhexidine 0.2%, mangosteen peel extract (Garcinia Mangostana L.) Table 2. The ANOVA One-way test results on the 2nd hour
Kelompok Average value ± Deviation standard
Aquadest 0.38 ± 0.0191
0.2% of chlorhexidine 0.39 ± 0.046
12.5% of mangosteen peel extract 0.25 ± 0.015
25% of mangosteen peel extract 0.30 ± 0.044
p-value 0.000
Table 3. The Tukey’s range test results
The 2nd-hour treatment The 4th-hour treatment The 6th-hour treatment
A C 12.5% of mangosteen peel extract : 12.5% of mangosteen peel extract
25% of mangosteen peel extract : 25% of mangosteen peel extract
* : Signiicant (< 0.05)
12,5% and Mangostana leaf mangosteen extract (25%) there was a very signiicant diference
which has the potential to decrease the size of
inlammation in rat gingiva. The positive control group given 0.2% chlorhexidine compared with the aquadest group, mangosteen peel extract (Garcinia Mangostana L.) 12.5% and Mangostana leaf mangosteen extract (25%) of mangosteen extract (Garcinia Mangostana L.) the potential to decrease the size of inlammation in rat gingiva. DISCUSSION
This research was conducted on mangosteen skin extract (Garcinia mangostana L.) 12,5% and
mangosteen peel extract (Garcinia mangostana
L.) 25% had very signiicant diference with positive control of chlorhexidine 0,2% and negative control of aquadest at hour to - 2, 4 and 6, whereas no signiicant diference was found between mangosteen leaf extract group (Garcinia mangostana L.) 12,5% with 25% mangosteen peel extract (Garcinia mangostana L.) at 2, 4 and 6 hours. Based on the above data, it can be
concluded that mangosteen peel extract (Garcinia
Mangostana L.) 12.5% has the strongest potential of monitoring the 2nd, 4th and 6th hours.
This study is in accordance with research conducted by Ni Wayan Arini on the efectiveness
of gourd mangosteen leather rinse after oral
physiotherapy for gingivitis healing that in the
gargling treatment group using mangosteen peel
stew water showed that 14 samples (87.5%) experienced healing and two sample (12.5%) the severity of gingivitis decreased with moderate category became mild. Active components contained in the skin of mangosteen, namely α-mangostin, β-mangostin, and methoxy-β-mangostin, eicacious to cure gingivitis.8
On the skin of mangosteen fruit found xanthone substances containing xanthone
compounds with the main compounds alpha
mangostin and gamma-mangostin, which is believed to have antioxidant, antibacterial, and anti-inlammatory.11,12 In addition to
xanthone, mangosteen skin also contains tannins and catechins. Tanin is known to have anti-inlammatory, astringent, antidiarrheal, diuretic, and antiseptic activity. Cathecin which also belongs to the lavonoid group also has
anti-inlammatory efect.13
Xanthone can suppress inlammatory processes by inhibiting cyclooxygenase enzymes and lipoxygenase enzymes. Inhibition of
cyclooxygenase enzymes and lipoxygenase
enzymes results in the release of prostaglandins, prostacyclins, thromboxanes, and leukotrienes also reduced so as to suppress inlammatory processes that can be marked by a decrease in the number of inlammatory cells. Other content in the skin of mangosteen fruit that has pharmacological activity as an anti-inlammatory is cathecin which belongs to lavonoid group. The mechanism of lavonoids in lowering the inlammatory process is by inhibiting the release of arachidonic acid, the
secretion of lysosomal enzymes from neutrophil
cells and endothelial cells, and inhibits the exudation phase of the inlammatory process.
Flavonoids inhibit the cyclooxygenase enzyme irreversibly (prostaglandin synthetase),
which catalyzes the change of arachidonic acid
into endoperoxide compounds thereby decreasing
the formation of prostaglandins which in turn will
reduce the inlammatory process. Reduction of the inlammatory process results in a decrease in the number of neutrophil cells. Thus, mangosteen peel extract (Garcinia Mangostana L.) is efective for the healing of inlammation of the gingiva.14
As inlammation enters the healing process, ibroblasts migrate immediately into the wound,
proliferate and produce collagen matrices to
repair damaged tissue. Fibroblasts are cellular
elements that are commonly found in wound
healing and repair of damaged tissue.15
CONCLUSION
The mangosteen peel extract at the concentration of 12.5% and 25% were efectively used in accelerating the inlammatory healing process of the mouse gingival due to its strong anti-inlammatory efect.
REFERENCES
Efektivitas Berkumur Air Rebusan Kulit Buah Manggis Untuk Penyembuhan Gingivitis pada Pasien Pasca Scaling. Jurnal Skala Husada. Apr 2014;11(1): p. 41-45.
3. Nadiawati RP. Efek Aplikasi Gel Ekstrak Kulit Manggis (Garcinia Mangostana L.) Terhadap Kepadatan Serabut Kolagen Pada Proses Penyembuhan Luka Gingiva (Kajian Pada Rattus Norvegicus) [minor thesis]. Yogyakarta: UGM; 2013.
4. Setianing Y. Pengaruh Obat Kumur Ekstrak Kulit Manggis (Garcinia Mangostana L ) Terhadap Jumlah Koloni Bakteri Cairan Sulkus Gingiva Pada Pasien Gingivitis [minor thesis]. Yogyakarta: UGM; 2015.
5. National Institute of Health Research and Development (NIHRD). Indonesia Basic Health Research (RISKESDAS) 2007-2008. Jakarta: Ministry of Health Republic of Indonesia; 2008. 6. Jurnal Kedokteran Gigi [homepage on
internet]. Informasi Seputar Kesehatan Gusi; c2012 [cited Nov 21 2012]; [about 5 screens]. Available from: http://www. jurnalkedokterangigi.com/post/read/483/ informasi-seputar-penyakit-gusi.html
7. Yulia AR. Pengaruh Ekstrak Kulit Buah Manggis (Garcinia Mangostana L.) Terhadap Jumlah Fibroblas Pada Gingiva Tikus Wistar Jantan Pasca Induksi Porphyromonas Gingivalis [minor thesis]. Jember: Unej; 2013.
8. Arini NW, Astuti SAPD, Nahak MM. Efektivitas Kumur-Kumur Air Rebusan Kulit Buah Manggis Pasca Oral Fisioterapi Untuk Penyembuhan Gingivitis. Jurnal Skala Husada. Apr 2014;11(1): p. 6-10.
9. Torres-Lagares D, Gutierrez-Perez JL, Hita-Iglesias P, Magallanes-Abad N, Flores-Ruiz R,
Basallote-Garcia M, et al. Randomized, Double-Blind Study Of Efectiveness Of Intra-Alveolar Application Of Chlorhexidine Gel In Reducing Incidence Of Alveolar Osteitis And Bleeding Complications In Mandibular Third Molar Surgery In Patients With Bleeding Disorders. J Oral Maxillofac Surg. Jun 2010;68(6): p. 1322-6. DOI: 10.1016/j.joms.2009.08.022.
10. Nakatani K, Nakahata N, Arakawa T, Yasuda H, Ohizumi Y. Inhibition of cyclooxygenase and prostaglandin E2 synthesis by gamma-mangostin, a xanthone derivative in mangosteen, in C6 rat glioma cells. Biochem Pharmacol. Jan 1, 2002;63(1): p. 73-9.
11. Mardawati E, Filianty F, Marta H. Kajian Aktivitas Antioksidan Ekstrak Kulit Manggis (Garcinia Mangostana L) Dalam Rangka Pemanfaatan Limbah Kulit Manggis Di Kecamatan Puspahiang Kabupaten Tasikmalaya. Jurnal Teknotan. 2008;2(3): p.
12. Nurchasanah. Khasiat Sakti Manggis Tumpas Berbagai Penyakit. Jakarta: Dunia Sehat; 2013. p. 84-5
13. Agni N. Respons Anti Inlamasi Ekstrak Kulit Buah Manggis (Garcinia Mangostana L.) Terhadap Jumlah Limfosit Pada Gingiva Tikus Wistar Jantan Pasca Diinduksi [minor thesis]. Jember: Unej; 2013.
14. Putri FI. Respons Antiinlamasi Ekstrak Kulit
Buah Manggis (Garcinia Mangostana Linn)
Terhadap Jumlah Sel Neutroil Pada Gingiva Tikus Wistar Jantan Pasca Diinduksi Oleh Porphyromonas Gingivalis. Jurnal Kedokteran Gigi [minor thesis]. Jember: Unej; 2013. 15. Newman MG, Takei HH, Klokkevold PR, Carranza
FA. Carranza’s Clinical Periodontology. 12th ed.