HALAMAN PENGESAHAN
PRA USULAN PENELITIAN UNGGULAN PRODI
Judul Penelitian : Analisis Biaya Pengobatan Penyakit Dengan Prevalensi Tinggi Sebagai Pertimbangan Dalam Penetapan
Nama Rumpun Ilmu: Farmasi Klinik
LAPORAN PENELITIAN UNGGULAN PRODI
ANALISIS BIAYA PENGOBATAN STROKE SEBAGAI PERTIMBANGAN DALAM PENETAPAN PEMBIAYAAN KESEHATAN BERDASAR INA-CBGs
DI ERA JAMINAN KESEHATAN NASIONAL 2014 BERDASARKAN PERMENKES NO. 69 TAHUN 2013
TIM PENGUSUL :
Ingenida Hadning, M.Sc., Apt. (19850304201004173122/0504038501)
Bangunawati Rahajeng, M.Si., Apt (19701105201110173154/0505117002)
Indriastuti Cahyaningsih, M.Sc., Apt (19850526201004173121/0526058501)
Pinasti Utami, M.Sc., Apt. (19850318201004173123/0518038501)
DAFTAR ISI
Hal
Halaman Pengesahan ... 2
Daftar Isi... 3
Ringkasan... 4
Pendahuluan... 4
Kelayakan Teknis... 5
Metode dan Mekanisme Alih Teknologi/desiminasi dan atau Intervensi Sosial... 7
Pemanfaatan Hasil ... 8
Organisasi dan Personil Pelaksana Kegiatan ... 9
Pembahasan ... Keterbatasan Penelitian ………... Kesimpulan ………... Saran ………... 49
50
51
Jadwal Kegiatan ... 52
Indikator Keberhasilan ... 52
Daftar Pustaka ... 53
RINGKASAN
Pemberlakuan tarif INA-CBG’s pada pembiayaan pasien stroke peserta JKN di seluruh rumah sakit di Indonesia menuntut pihak rumah sakit untuk dapat melakukan kendali mutu dan biaya perawatan seefisien mungkin. Penelitian ini bertujuan untuk mengetahui rerata biaya riil pengobatan pasien stroke rawat inap di RS PKU Muhammadiyah Yogyakarata dan perbedaanya dengan tarif INA-CBG’s berdasarkan Permenkes No. 69 Tahun 2013.
Penelitian dilakukan secara observasional dengan desain cross sectional. Pengambilan data dilakukan secara retrospektif dengan subjek penelitian adalah seluruh populasi pasien stroke rawat inap peserta JKN yang memenuhi kriteria inklusi dan eksklusi penelitian yang terdaftar dari bulan Januari - Juni 2014. Data penelitian berupa direct medical cost yang dianalisis kesesuaiannya dengan tarif INA-CBG’s. Analisis data dilakukan dengan uji statistik t test.
Rerata biaya riil pasien rawat inap untuk kelas I dengan kode G-4-14-I sebesar Rp. 6.175.260,- ± Rp. 3.641.107,-, G-4-15-I sebesar Rp.10.260.320,- ± Rp.7.107.732,-, G-4-15-II sebesar Rp.7.692.475,- ± Rp.2.339.329,-, G-4-15-III sebesar Rp.11.318.550,- ± Rp.9.457.199,-. Kelas II dengan kode G-4-13-I sebesar Rp 8.078.200,-, G-4-14-I sebesar Rp 3.705.700,-, G-4-14-II sebesar Rp 3.719.950,- ± Rp 1.591.202,-, G-4-15-I sebesar Rp 3.957.000,-, G-4-15-II sebesar Rp 6.095.950,- ± Rp 3.114.451,-. Kelas III dengan kode INA-CBG’s G-4-13-I sebesar Rp 4.074.000,-, I sebesar Rp 1.881.600,- ± Rp 454.952,-, G-4-14-II sebesar Rp 1.593.262,- ± Rp 666.908,-, G-4-15-I sebesar Rp 2.817.880,- ± Rp 1.240.742,-, G-4-15-II sebesar Rp 2.211.500,- ± Rp 1.223.001,-. Pada kelas I dan II, secara statistik tidak terdapat perbedaan yang signifikan antara rerata biaya riil dengan tarif INA-CBG’s. Pada kelas III terdapat perbedaan yang signifikan pada kode G-4-14-II dan G-4-15-II, namun tidak terdapat perbedaan yang signifikan pada kode G-4-14-I dan G-4-15-I. Dalam penelitian ini dapat disimpulkan tidak terdapat perbedaan yang signifikan antara rerata biaya riil dengan tarif INA-CBG’s. RS PKU Muhammadiyah Yogyakarta telah mampu mengelola tarif INA-CBG’s penyakit stroke rawat inap yang ditetapkan oleh pemerintah.
PENDAHULUAN
Dengan diberlakukannya Peraturan Presiden RI No.12 Tahun 2013 tentang Jaminan Kesehatan yang diselenggarakan oleh Badan Penyelenggara Jaminan Sosial Kesehatan (BPJS Kesehatan) dimana mulai 1 Januari 2014 semua penduduk Indonesia akan memperoleh jaminan berupa perlindungan kesehatan berupa manfaat pemeliharaan kesehatan dan perlindungan dalam memenuhi kebutuhan dasar kesehatan, maka untuk pembayaran fasilitas kesehatan bagi pasien rawat inap BPJS Kesehatan melakukan pembayaran berdasarkan Indonesian Case Based Groups (INA-CBG’s). Dalam sistem INA-CBGs komponen biaya yang ditanggung oleh pihak BPJS Kesehatan terdiri atas biaya perawatan, penginapan, tindakan, obat-obatan, penggunaan alat kesehatan, dan jasa yang dihitung terpadu dalam paket. Dengan demikian analisis biaya pengobatan rawat inap sangat dibutuhkan dalam perencanaan pengobatan. Hasil penelitian diharapkan dapat memberi gambaran mengenai kemampuan rumah sakit dalam mengendalikan biaya pengobatan sesuai tarif pelayanan kesehatan yang berlaku dalam penyelenggaraan program jaminan kesehatan 2014 serta dapat dijadikan salah satu evaluasi pelaksanaan program jaminan kesehatan di Indonesia.
Rumusan Masalah : Seperti apakah kesesuaian biaya riil pengobatan penyakit stroke bagi pasien rawat inap di Rumah Sakit PKU Muhammadiyah Yogyakarta dengan besarnya pembiayaan kesehatan berdasarkan Permenkes RI No 69 Tahun 2013 tentang Standar Tarif Pelayanan Kesehatan Pada Fasilitas Kesehatan Tingkat Pertama dan Tingkat Lanjutan Dalam Penyelenggaraan Program Jaminan Kesehatan?
Pertama dan Tingkat Lanjutan Dalam Penyelenggaraan Program Jaminan Kesehatan.
Lokasi kegiatan : Rumah Sakit PKU Muhammadiyah Yogyakarta dan Program Studi Farmasi FKIK UMY.
KELAYAKAN TEKNIS
Beragam guideline pengobatan penyakit stroke menyebabkan beragam pula jumlah biaya yang harus dibayar oleh penderita atau keluarga penderita atau pihak BPJS Kesehatan. Bila penanganan atau pemilihan obat tidak tepat maka dapat menyebabkan waktu tinggal di rumah sakit menjadi lebih lama atau terjadinya komplikasi yang lain yang pada akhirnya akan terjadi pembengkakan biaya. Besarnya biaya pengobatan selain dipengaruhi oleh jenis terapi obat yang digunakan juga dipengaruhi oleh jenis tindakan yang diberikan tenaga medis, keahlian tim medis dalam mendiagnosis secara cepat dan tepat, serta kepatuhan tenaga medis terhadap clinical pathway yang telah ditetapkan rumah sakit sebelumnya. Dalam sistem INA-CBGs komponen biaya yang ditanggung oleh pihak asuransi kesehatan terdiri atas biaya perawatan, penginapan, tindakan, obat-obatan, penggunaan alat kesehatan, dan jasa yang dihitung terpadu dalam paket. Dengan diberlakukannya INA-CBGs pada pembiayaan rumah sakit, maka analisis biaya pengobatan rawat inap sangat dibutuhkan dalam perencanaan pengobatan sehingga rumah sakit dapat melakukan penghematan biaya agar rumah sakit tidak merugi. Analisis biaya tersebut selain berguna dalam hal mengajukan klaim kepada pihak asuransi kesehatan juga dapat digunakan dalam memberikan pengobatan yang tepat bagi pasien berdasarkan data biaya pengobatan.
Penelitian dilakukan dengan tahapan sebagai berikut : 1. Tahap persiapan
Tahapan ini meliputi pengurusan ijin serta persiapan lembar pencatatan data pasien dan lembar pencatatan biaya pengobatan stroke.
Pelaksanaan penelitian dilakukan dalam bentuk kegiatan :
a. Review rekam medik di rumah sakit untuk mendapatkan data karakteristik demografi yang meliputi nama pasien, nomor rekam medik, usia, jenis kelamin pasien; lama dirawat di rumah sakit (tanggal dan jam masuk-keluar rumah sakit), tanggal dan jam serangan, faktor resiko, catatan penggunaan obat, catatan keperawatan, hasil uji laboratorium yang telah dilakukan, dan hasil terapi yang diukur dari indek barthel. Semua data tersebut dicatat dalam lembar pencatatan data pasien.
b. Penelusuran biaya terapi pasien stroke berdasarkan data rekam medis pasien. Biaya penggunaan obat dan alat kesehatan ditelusuri dari instalasi farmasi rumah sakit, sedangkan tarif biaya tindakan medis, biaya perawatan, biaya pemeriksaan penunjang (biaya laboratorium, fisioterapi, dan gizi), biaya administrasi, biaya penunggu pasien dan sewa ruangan, biaya kartu berobat, dan biaya karcis ditelusuri dari bagian administrasi keuangan.
3. Tahap pengolahan dan analisis data
Data dari rekam medis pasien dan data dari penelusuran biaya pengobatan pasien setelah terkumpul akan dilakukan pengolahan dan analisis data sesuai metode analisis yang digunakan.
Penelitian ini akan dilakukan berkesinambungan dengan melibatkan beberapa rumah sakit yang mengikuti program Jaminan Kesehatan Nasional (JKN) dan meneliti penyakit yang lebih luas. Hasilnya diharapkan dapat dijadikan sebagai salah satu evaluasi pelaksanaan program jaminan kesehatan di Indonesia.
METODE DAN MEKANISME ALIH TEKNOLOGI/DISEMINASI DAN ATAU INTERVENSI SOSIAL
Penelitian ini merupakan penelitian observasional dengan rancangan penelitian cross sectional menurut perspektif rumah sakit. Metode pengambilan data secara retrospektif. Subyek penelitian yang digunakan adalah seluruh populasi pasien rawat inap peserta JKN di Rumah Sakit PKU Muhammadiyah Yogjakarta yang menderita penyakit stroke dari bulan Januari - Juni 2014 yang memenuhi kriteria inklusi penelitian dan telah dikelompokkan berdasarkan INA-CBGs. Analisis data dilakukan dengan uji statistik MannWhitney.
Hasil penelitian diharapkan dapat memberi gambaran mengenai kemampuan rumah sakit dalam mengendalikan biaya pengobatan sesuai tarif pelayanan kesehatan yang berlaku dalam penyelenggaraan program jaminan kesehatan 2014 serta dapat dijadikan acuan bagi BPJS Kesehatan dalam mengambil kebijakan.
PEMANFAATAN HASIL
Strategi Pemanfaatan Hasil Kegiatan :
1. Hasil penelitian akan diterbitkan pada jurnal ilmiah dan dipresentasikan di forum-forum ilmiah.
2. Hasil penelitian akan diberikan kepada rumah sakit terkait dan BPJS kesehatan.
Intervensi sosial yang dapat memperbaiki karakter bangsa : Hasil penelitian diharapkan dapat bermanfaat bagi rumah sakit dengan memberi gambaran mengenai kemampuan rumah sakit dalam mengendalikan biaya pengobatan sesuai tarif pelayanan kesehatan yang berlaku dalam penyelenggaraan program jaminan kesehatan 2014 serta dapat dijadikan acuan bagi BPJS Kesehatan dalam mengambil kebijakan.
STRATEGI PELEMBAGAAN INDUSTRIALISASI KE ARAH KARAKTER BANGSA
(tidak ada)
ORGANISASI DAN PERSONIL PELAKSANA KEGIATAN TABEL 1. Organisasi dan Profil
Ingenida Hadning
Bangunawati Rahajeng
Indriastuti Cahyaningsih
Pinasti Utami
Gelar M.Sc., Apt M.Si., Apt M.Sc., Apt M.Sc., Apt
Jenis Kelamin Wanita Wanita Wanita Wanita
Unit Kerja Farmasi Farmasi Farmasi Farmasi
Bidang
Keahlian/Tugas
Manajemen Farmasi/Ketua Peneliti
Farmasi Klinik/Peneliti
Farmasi Klinik/Peneliti
Farmasi Klinik/Peneliti
Pendidikan terakhir
S2 S2 S2 S2
Alokasi waktu 16 jam/mgg 16 jam/mgg 16 jam/mgg 16 jam/mgg
PEMBAHASAN
Stroke Patient Characteristic at Jogja Hospital
During January – June 2014 there were 49 stroke patients at PKU Muhammadiyah Yogyakarta Hospital who fulfilled the inclusion criteria. There were 2 patients with code I619 (Intra-cerebral Hemorrhage), 20 patients with code I639 (Cerebral Infarction), and 27 patients with code I64 (Unspecified Stroke). Stroke patient characteristic can be seen on the table 1 as below.
Characteristics
Intra-cerebral Hemorrhage (I619)
Cerebral Infarction (I639)
Unspecified Stroke (I64)
(n=2) % (n=20) % (n=27) %
Sex:
Male 1 50 14 70 19 70
Female 1 50 6 30 8 30
Age :
≤ 55 years of
age 0 0 4 13 3 7
> 55 years of
age 2 100 9 27 13 30
Most of stroke patient with diagnosis code of I619 (Intra-cerebral Hemorrhage), I639 (Cerebral Infarction), and I64 (Unspecified Stroke) were aged 55. It might be due to the risk of stroke will increase 2 times after age 55 [11]. At the elderly group, the risk of hypertension increases because the blood vessels become more rigid and less elastic [12], whereas the hypertension is the most important risk factor of stroke [13] [14]. According to the result of stroke patient’s case study with cerebral infarction (I639) and non-specific stroke cases (I64), it has been known that male has higher stroke prevalence than female (70% and 30%). According to [4], men have higher risk to get stroke compared to women in the same age. It is caused by women’s hormones that have protective roles toward the diseases related to blood artery [15]. Furthermore, man also have higher potential to get stroke because of their life style like smoking, staying up to work, and high rate of stress [16].
One of the factors affecting the length of stay in acute ischemic stroke patients was age of 65 years or more [17]. Another study stated an increase of length of stay in diabetic patients with the age of 60 years or more, and a decrease of length of stay in female patients [18].
Costs Analysis Based on INA-CBGs
are input by hospital coding officer along with Jamkesmas reporting in each day through hospital-owned INA CBGs software [19] [20] [21]. The average cost of patient care based on the average length of stay can be seen on Table 2 as below.
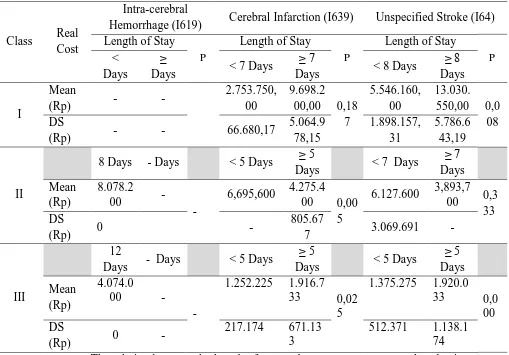
Tabel 2. The average cost of patient care based on the average length of stay with JKN membership at PKU Muhammadiyah Yogyakarta Hospital
during January 2014 – June 2014
Class Real Cost
Intra-cerebral
Hemorrhage (I619) Cerebral Infarction (I639) Unspecified Stroke (I64) Length of Stay
P
Length of Stay
P
Length of Stay
P <
Days
≥
Days < 7 Days
≥ 7
Days < 8 Days
≥ 8 Days
I
Mean
(Rp) - -
2.753.750, 00
9.698.2 00,00 0,18
7
5.546.160, 00
13.030. 550,00 0,0
08 DS
(Rp) - - 66.680,17
5.064.9 78,15 1.898.157, 31 5.786.6 43,19 II
8 Days - Days < 5 Days ≥ 5
Days < 7 Days
≥ 7 Days Mean
(Rp)
8.078.2
00 -
-
6,695,600 4.275.4 00 0,00
5
6.127.600 3,893,7 00 0,3
33 DS
(Rp) 0 -
805.67
7 3.069.691 -
III
12
Days - Days < 5 Days
≥ 5
Days < 5 Days
≥ 5 Days
Mean (Rp)
4.074.0
00 -
-
1.252.225 1.916.7 33 0,02
5
1.375.275 1.920.0 33 0,0
00 DS
(Rp) 0 -
217.174 671.13 3
512.371 1.138.1 74 The relation between the length of stay and treatment cost was analysed using Pearson and Spearman correlation test. Based on bivariat corelation analysis stroke with diagnose code I639 (Cerebral Infarction) with p value is <0,05 for class II (0,005) and III (0,025) and > 0,05 for class I (0,187), and diagnose code I64 (Unspecified Stroke) with p value is <0,05 for class I (0,008) and III (0,000) and > 0,05 for class II (0,333). Those diagnose codes have positive correlation coefficient, and it can be concluded that there is a positive correlation between the length of stay and treatment cost which means the longer the patient stay the higher treatment cost would be [9] [17] [22].
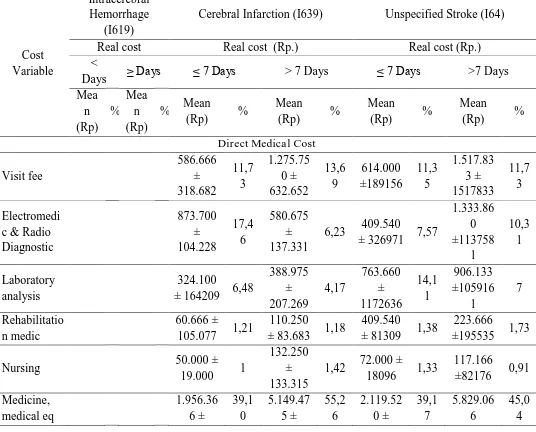
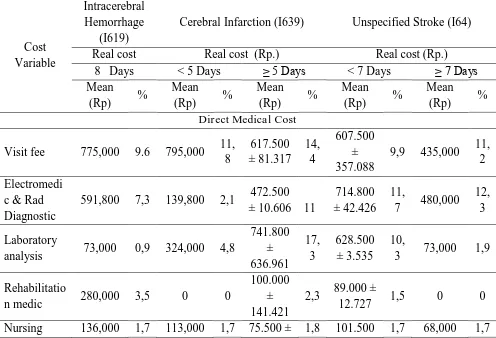
medical
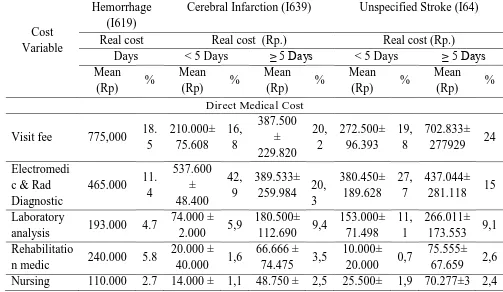
and non-medical costs as seen in Table 3. The greatest components of stroke treatment cost from all the diagnostic codes and all class for direct medical cost were medicine cost and medical equipment cost (Rp 859.333 to Rp 5.829.066), visite fee (Rp 210.000 to Rp 1.517.000), and electro medic and radiology diagnostic cost (Rp 139.800 to Rp 1.333.860), and the greatest component of direct non medical cost were room cost (Rp 150.000 to Rp 2.907.500).
Table 3. Details of Direct Medical and Non-Medical Cost Stroke Patient Treatment class I with JKN Membership at PKU Muhammadiyah Yogyakarta Hospital
Cost Variable
Intracerebral Hemorrhage
(I619)
Cerebral Infarction (I639) Unspecified Stroke (I64)
Real cost Real cost (Rp.) Real cost (Rp.)
<
Days ≥ Days ≤ 7 Days > 7 Days ≤ 7 Days >7 Days Mea n (Rp) % Mea n (Rp)
% Mean
(Rp) %
Mean
(Rp) %
Mean
(Rp) %
Mean
(Rp) %
Direct Medical Cost
Visit fee 586.666 ± 318.682 11,7 3 1.275.75 0 ± 632.652 13,6 9 614.000 ±189156 11,3 5 1.517.83 3 ± 1517833 11,7 3 Electromedi c & Radio Diagnostic 873.700 ± 104.228 17,4 6 580.675 ± 137.331
6,23 409.540
± 326971 7,57
1.333.86 0 ±113758 1 10,3 1 Laboratory analysis 324.100
± 164209 6,48
388.975 ± 207.269 4,17 763.660 ± 1172636 14,1 1 906.133 ±105916 1 7 Rehabilitatio n medic 60.666 ±
105.077 1,21
110.250
± 83.683 1,18
409.540
± 81309 1,38
223.666
±195535 1,73
Nursing 50.000 ±
19.000 1
132.250 ± 133.315
1,42 72.000 ±
18096 1,33
117.166
±82176 0,91
2.497.17 7
5.013.34 2
1170054 ±291631
4
Nutrition 0 0 4.375 ±
8.750 0,05 0 0 0 0
Direct Non Medical Cost
Room 1.046.66 6 ± 761.090 20,9 2 1.545.62 5 ± 617.124 16,5
9 1.272.40 0 ± 635182 23,5 1 2.907.50 0 ±137832 4 22,4 7 Administrati on 105.000
± 22.516 2,1
131.375 ± 72.269
1,41 85.640 ±
20526 1,58
106.573 ± 22847
0,82
Total 5.003.16
4 100
9.318.75
0 100
5.411.56
0 100
12.941.7
97 100
Table 4. Details of Direct Medical and Non-Medical Cost Stroke Patient Treatment class II with JKN Membership at PKU Muhammadiyah Yogyakarta Hospital
Cost Variable
Intracerebral Hemorrhage
(I619)
Cerebral Infarction (I639) Unspecified Stroke (I64)
Real cost Real cost (Rp.) Real cost (Rp.)
8 Days < 5 Days ≥ 5 Days < 7 Days ≥ 7 Days Mean
(Rp) %
Mean
(Rp) %
Mean
(Rp) %
Mean (Rp) %
Mean
(Rp) % Direct Medical Cost
Visit fee 775,000 9.6 795,000 11, 8 617.500 ± 81.317 14, 4 607.500 ± 357.088
9,9 435,000 11, 2
Electromedi c & Rad Diagnostic
591,800 7,3 139,800 2,1 472.500 ± 10.606 11
714.800 ± 42.426
11,
7 480,000 12,
3
Laboratory
analysis 73,000 0,9 324,000 4,8
741.800 ± 636.961 17, 3 628.500 ± 3.535 10,
3 73,000 1,9
Rehabilitatio
n medic 280,000 3,5 0 0
100.000 ± 141.421
2,3 89.000 ±
12.727 1,5 0 0
17.677 ± 19.091 Medicine, medical eq 4,145,40 0 51, 3 4,332,30 0 64, 7 1.314.10 0 ± 1.234.04 2 30, 7 2.575.75 0 ± 2.002.59 7
42 1,626,10 0
41, 8
Nutrition 0 0 0 0 6.250 ±
8.838
0,1
5 0 0 0 0
Direct Non Medical Cost
Room 2,000,00
0
24,
8 900,000 13, 4 862.500 ± 159.099 21, 2 1.332.50 0 ± 696.500 21, 7 1,120,00 0 28, 8 Administrati
on 77,000 0,9 91,500 1,4
85.250 ± 8.838
2 78.050 ±
19.021 1,3 91,600 2,4
Total 8.078.20 0 10 0 6.695.60 0 10 0 4.275.40 0 10 0 6.127.60 0 10 0 3.893.70 0 10 0
Table 5. Details of Direct Medical and Non-Medical Cost Stroke Patient Treatment class III with JKN Membership at PKU Muhammadiyah Yogyakarta Hospital
Cost Variable
Intracerebral Hemorrhage
(I619)
Cerebral Infarction (I639) Unspecified Stroke (I64)
Real cost Real cost (Rp.) Real cost (Rp.)
Days < 5 Days ≥ 5 Days < 5 Days ≥ 5 Days Mean
(Rp) %
Mean
(Rp) %
Mean
(Rp) %
Mean
(Rp) %
Mean
(Rp) % Direct Medical Cost
Visit fee 775,000 18. 5 210.000± 75.608 16, 8 387.500 ± 229.820 20, 2 272.500± 96.393 19, 8 702.833± 277929 24
Electromedi c & Rad Diagnostic
465.000 11. 4 537.600 ± 48.400 42, 9 389.533± 259.984 20,
3 380.450± 189.628 27, 7 437.044± 281.118 15
Laboratory
analysis 193.000 4.7
74.000 ± 2.000 5,9
180.500± 112.690 9,4
153.000± 71.498
11, 1
266.011± 173.553 9,1 Rehabilitatio
n medic 240.000 5.8
20.000 ± 40.000 1,6
66.666 ± 74.475 3,5
10.000± 20.000 0,7
19.339 22.044 16.114 3.155 Medicine, medical eq 1.409.00 0 34. 6 173.500 ± 89.302 13, 9 429.783± 218.512 22, 4 270.050± 222.917 19, 6 859.333± 749.244 29, 4
Nutrition 0 0 0 0 0 0 0 0
Direct Non Medical Cost
Room 825.000 20.
3
150.000 ± 61.237 12
337.500± 155.523 17, 6 187.500± 43.301 13, 6 433.333± 97.628 14, 8 Administrati
on 77.000 1.9
73.125 ± 7.750 5,8
76.500 ± 1.224
4 76.275± 1.517 5,5
75.644± 4.179
2,6
Total 4.074.00 0 10 0 1.252.22 5 10 0 1.916.73 2 10 0 1.375.27 5 10 0 2.920.03 0 10 0
The costs of medicine and medical equipment, visite fee, and electromedic and radiology diagnostic cost were affected by the accuracy of diagnosis, treatment selection, and stroke comorbidities factors [9] [17] [22] [23]. Those factors then will directly affect the patient’s length of stay and treatment cost as seen on Table 2.
Other studies have concluded that the length of stay for ischemic stroke patient in Sardjito Hospital was affected by stroke severity [9]. The difference in length of stay of general disease was affected by the disease severity and comorbid factor such as myocardial infarction and congestive heart failure [22] [24] [25] [26]. Some factors that might lengthen the hospitalization of acute ischemic stroke patients were diabetes mellitus, atrial fibrillation, type of stroke, stroke treatment, and stroke relaps [17].
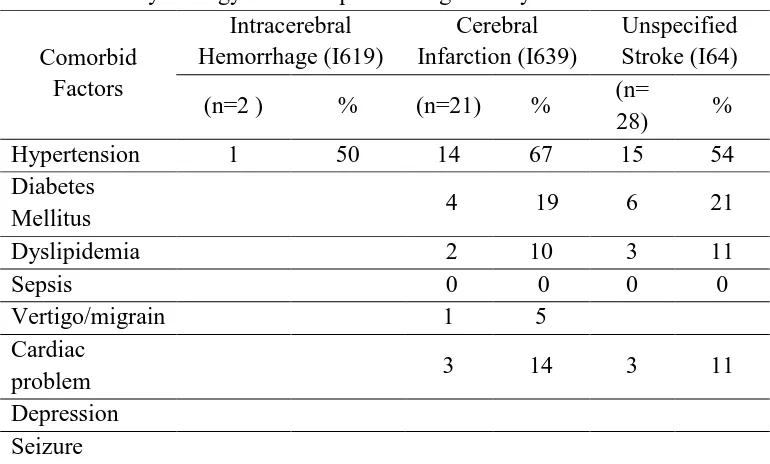
The stroke therapy costs for all diagnose codes at PKU Muhammadiyah Yogyakarta Hospital are not only affected by the type and number of drugs used but also affected by other additional medications to treat the stroke comorbid factors. The more type of drugs used for stroke treatment the higher the treatment cost should be. Moreover, the more comorbid factors the higher the treatment cost should be as well [9] [17] [22] [23].
Table 6. Stroke comorbid factors of Jamkesmas membership at PKU Muhammadiyah Yogyakarta hospital during January–June 2014
Comorbid Factors
Intracerebral Hemorrhage (I619)
Cerebral Infarction (I639)
Unspecified Stroke (I64)
(n=2 ) % (n=21) % (n=
28) %
Hypertension 1 50 14 67 15 54
Diabetes
Mellitus 4 19 6 21
Dyslipidemia 2 10 3 11
Sepsis 0 0 0 0
Vertigo/migrain 1 5
Cardiac
problem 3 14 3 11
Depression
Seizure
Hypertension might cause intracranial vessel rupture or become stenotic. The ruptur vessel will cause intracranial haemorrhage, but when the the vessel become stenotic it might disturb intracranial blood flow and, eventually, brain cellular death. Moreover, the rise in blood pressure might faster the plaque formation process, endothelial layer damage, and finally plaque would be prone to rupture and causes thrombus. Thrombus then will occlude blood vessel locally, or become emboly in blood stream into cerebrovascular system [12].
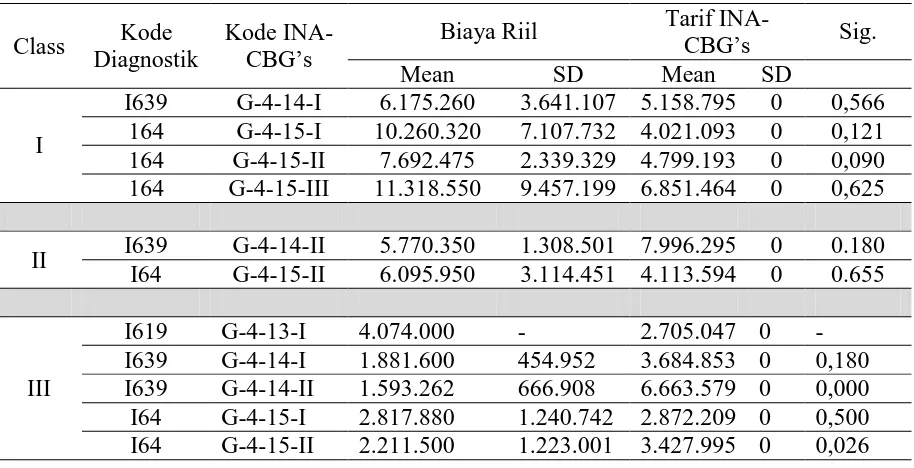
Table 7. Correlation Between Real Cost and INA-CBGs Cost
Class Kode Diagnostik
Kode
INA-CBG’s Biaya Riil
Tarif
INA-CBG’s Sig.
Mean SD Mean SD
I
I639 G-4-14-I 6.175.260 3.641.107 5.158.795 0 0,566 164 G-4-15-I 10.260.320 7.107.732 4.021.093 0 0,121 164 G-4-15-II 7.692.475 2.339.329 4.799.193 0 0,090 164 G-4-15-III 11.318.550 9.457.199 6.851.464 0 0,625
II I639 G-4-14-II 5.770.350 1.308.501 7.996.295 0 0.180 I64 G-4-15-II 6.095.950 3.114.451 4.113.594 0 0.655
III
I619 G-4-13-I 4.074.000 - 2.705.047 0 - I639 G-4-14-I 1.881.600 454.952 3.684.853 0 0,180 I639 G-4-14-II 1.593.262 666.908 6.663.579 0 0,000 I64 G-4-15-I 2.817.880 1.240.742 2.872.209 0 0,500 I64 G-4-15-II 2.211.500 1.223.001 3.427.995 0 0,026
The amount of real stroke treatment cost at PKU Muhammadiyah Yogyakarta Hospital for diagnosis code of I639 and I64 in class I were averagely higher than the amount of INA-CBGs cost for the same diagnosis code and the same class. In class II the amount of real stroke treatment cost for diagnosis code of I639 were were averagely lower than the amount of INA-CBGs cost, while it was higher for diagnosis code of I64 for real stroke treatment. In class III the amount of real stroke treatment cost for diagnosis code of I619 were higher than the amount of INA-CBGs while it was lower for diagnosis code of I639 and I64 for real stroke treatment cost. Moreover, One Sample t test analysis for class I diagnose code I639 and I64 with p value was > 0.05, class II diagnose code I639 and I64 with p value was > 0.05, and class III diagnose code I639 (G-4-14-I) and I64 (G-4-15-I) with p value was > 0.05. That meant there was an insignificant discrepancies between real stroke treatment cost and the corresponding INA-CBG’s cost. In the other side One Sample t test analysis for class III diagnose code I639 (G-4-14-II) and I64 (G-4-15-II) with p value was < 0.05, that meant there was a significant discrepancies between real stroke treatment cost and the corresponding INA-CBG’s cost. According to the aforementioned analysis it was concluded that the hospital was adequately capable of doing rate management determined by INA-CBGs. By doing so, the hospital did not have to bear too many cost deficits [9].
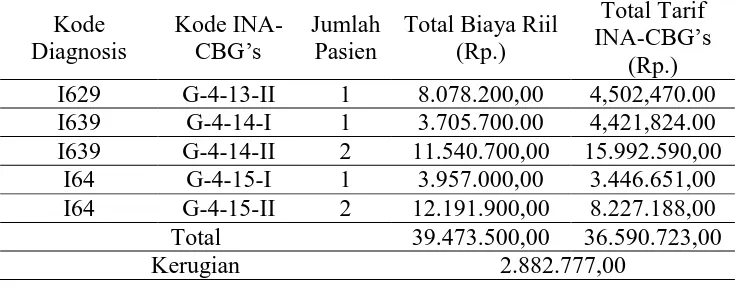
2015) for all stroke diagnosis codes and severity class I and II as much as Rp 59.104.642 and Rp 2.882.777. The cost deficits might actually be anticipated if its causes and solutions were known before. One of its possible causes were branded medicine prescribing that might actually be substituted with generic medicine eventhough some of the prescribing has already used generic medicine [9].
Table 8. Total Real Cost and INA-CBGs Rate for JKN Membership with Stroke class I at PKU Muhammadiyah Yogyakarta Hospital during January-June 2014
Kode Diagnosis
Kode
INA-CBG’s Jumlah Pasien
Total Biaya Riil (Rp.)
Total Tarif INA-CBG’s
(Rp.) I639 G-4-14-I 6 30.876.300,00 25.793.975,00 I639 G-4-14-II 1 5.587.000,00 9.329.010,00 I639 G-4-14-III 1 17.726.200,00 11.665.308,00
I64 G-4-15-I 5 51.301.600,00 20.105.465,00 I64 G-4-15-II 5 30.769.900,00 19.196.772,00 I64 G-4-15-III 2 22.637.100,00 13.702.928,00 Total 158.898.100,00 99.793.458,00
Kerugian 59.104.642,00
Table 9. Total Real Cost and INA-CBGs Rate for JKN Membership with Stroke class II at PKU Muhammadiyah Yogyakarta Hospital
during January-June 2014
Kode Diagnosis
Kode
INA-CBG’s Jumlah Pasien
Total Biaya Riil (Rp.)
Total Tarif INA-CBG’s
(Rp.) I629 G-4-13-II 1 8.078.200,00 4,502,470.00 I639 G-4-14-I 1 3.705.700.00 4,421,824.00 I639 G-4-14-II 2 11.540.700,00 15.992.590,00
I64 G-4-15-I 1 3.957.000,00 3.446.651,00 I64 G-4-15-II 2 12.191.900,00 8.227.188,00 Total 39.473.500,00 36.590.723,00
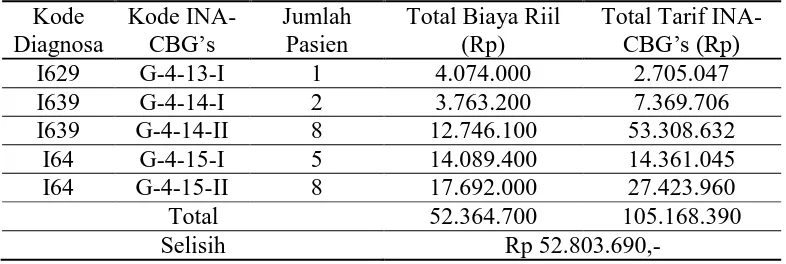
Table 10. Total Real Cost and INA-CBGs Rate for JKN Membership with Stroke class III at PKU Muhammadiyah Yogyakarta Hospital
during January-June 2014 Kode
Diagnosa
Kode
INA-CBG’s Jumlah Pasien
Total Biaya Riil (Rp)
Total Tarif INA-CBG’s (Rp)
I629 G-4-13-I 1 4.074.000 2.705.047
I639 G-4-14-I 2 3.763.200 7.369.706
I639 G-4-14-II 8 12.746.100 53.308.632
I64 G-4-15-I 5 14.089.400 14.361.045
I64 G-4-15-II 8 17.692.000 27.423.960
Total 52.364.700 105.168.390
Selisih Rp 52.803.690,-
The government-determined INA-CBGs code very depended with the diagnosis code reported by hospital coding officers, thus diagnosis writing accuracy and medical procedure writing completeness became the primary factors due to the discrepancy of INA-CBGs rate for every code and severity level determined by primary and secondary diagnosis and the medical procedures [9] [19] [21] [28]. This rate difference became the main problem in coding process. Management of PKU Muhammadiyah Yogyakarta Hospital had to socialize to doctors regarding the coding process and the importance of correct and detailed diagnosis writing that might cause inaccurate rate deciding. Thus, solving this problem might be a step to prevent hospital loss.
Based on the above discussion, there are some important factors to be concerned for managing JKN rate effectively: the accuracy of diagnosis, treatment decision and nursing care for the stroke’s treatment and also its comorbid factors. They are also important issues to avoid hospital’s financial loss. Hospital management is expected to demonstrate those important issues to their medical staffs and paramedics to reach the same level of understanding and commitment in the medical team at PKU Muhammadiyah Yogyakarta Hospital.
KETERBATASAN PENELITIAN Keterbatasan dari penelitian ini adalah
sebenarnya dan hanya bisa melihat dari data yang tertulis dalam rekam medis.
b. Klasifikasi severity dan biaya penggantian pengobatan penyakit stroke dalam sistem komputasi BPJS yang belum diketahui secara pasti.
KESIMPULAN DAN SARAN 1. Kesimpulan
Tidak ada perbedaan signifikan antara rata-rata biaya riil terapi stroke dengan pembiayaan kesehatan berdasarkan Permenkes Nomor 69 Tahun 2013, sehingga rumah sakit mampu mengelola pembiayaan terapi dengan optimal. 2. Saran
a. Perlu dilakukan penelitian lebih lama untuk mendapatkan jumlah sampel yang lebih banyak sehingga data yang diuji dapat lebih valid.
JADWAL KEGIATAN
No Kegiatan Bulan
I II III IV V VI VII VIII 1 Tahap Persiapan
a. Pengurusan ijin √
b. Persiapan lembar pencatatan biaya pengobatan pasien
√
2 Tahap Pelaksanaan
a. Penelusuran biaya penggunaan obat dan alat kesehatan dari instalasi farmasi rumah sakit
√ √ √ √
b. Penelusuran biaya tindakan medis, perawatan, pemeriksaan penunjang, administrasidan sewa ruangan dari bagian administrasi keuangan
√ √ √ √ √
3 Tahap Penyelesaian
a. Rekapitulasi data penelitian √
b. Pengolahan dan analisis data √
c. Penyusunan laporan akhir √
INDIKATOR KEBERHASILAN
Tuliskan indikator keberhasilan penelitian mengikuti tabel sebagai berikut :
Jenis Luaran
Capaian yang Ditargetkan*
No. Tahun I Tahun II Tahun III
1 Pelayanan jasa (status: pengembangan, uji coba, penerapan, evaluasi)
Analisis data Evaluasi hasil penelitian
Masukan bagi rumah sakit dan
BPJS 2 Kerja sama (status: penjajakan,
pelaksanaan, evaluasi kerja sama)
RS terkait & BPJS
RS terkait & BPJS
RS terkait & BPJS
DAFTAR PUSTAKA
Adams H.P, Jr, delZoppo G.J, vonKummer R, 2000, Management of Stroke: A Practical Guide for the Prevention, Evaluation and Treatment of Acute
Stroke, 1st ed, Caddo US: Professional Communications Inc.
Adams H.P, Jr, Adams R.J, Brott T, delZoppo G.J, Furlan A, Goldstein L.B, Grubb R.L, Higashida R, Kidwell C, Kwiatkwoski T.G, Marler J.R, Hademenos J, 2003, Guideline for the Early Management of Patient With Ischemic Stroke, Stroke 34:1056.
Anonim, 2007, Surat Keputusan Menteri Kesehatan Republik Indonesia Nomor 989/Menkes/SK/IX/2007tentang Pemberlakuan INA-DRG, Depkes RI, Jakarta.
Anonim, 2011, Peraturan Menteri Kesehatan Republik Indonesia Nomor
903/Menkes/PER/V/2011 tentang Pedoman Pelaksanaan Program
Jaminan Kesehatan Masyarakat, Depkes RI, Jakarta.
Anonim, 2013, Peraturan Menteri Kesehatan Republik Indonesia Nomor 69 tahun 2013 tentang Tarif Pelayanan Kesehatan Tingkat Lanjutan dalam
Anonim, 2013a, Peraturan Presiden Republik Indonesia Nomonr 12 tahun 2013 tentang Jaminan Kesehatan, Presiden RI, Lembaran Negara RI tahun 2013 nomor 29.
Anonim, 2001, Analisis Biaya Rumah Sakit, Modul 1 Seri Latihan Analisis Biaya Rumah Sakit, Departemen Kesehatan RI, Jakarta.
Anonim, 2011d, Pengenalan INA-CBGs Oleh Tim Centre for Casemix, Departemen Kesehatan RI, Jakarta..
Arikunto, S., 2005, Manajemen Penelitian, edisi VII, 234-262, Rineka Cipta, Jakarta.
Armilawaty, Amalia, H., Amiruddin, R., 2007, Hipertensi dan Faktor Risikonya dalam Kajian Epidemiologi, [Online], Artikel Ilmiah, Bagian Epidemiologi FKM UNHAS, www.jurnalpembahasan/hipertensi dan faktor risikonya dalam kajian epidemiologi”New Paradigm for Public Health”.htm, [2012, Desember 20].
Bootman, J.L., Towsend, R.J., and McGhan, W.F., 2005, Principles of Pharmacoeconomics, 3rd edition, Harvey Whitney Books Company : USA, 315-327.
Broderick J.P, Adams H.P, Adams Jr, Barsan W, Feinberg W, Feldmann E, Grotta J, Kase C, Kreiger D, Mayberg M, Tilley B, Zabramski J.M, Zuccarello M, 1999, Guidelines for Management of Spontaneous Intracerebral Hemorrhage, Stroke; 30:905-915.
Chobanian, A.V., Bakris, G. L., Black, H. R., Cushman, W. C., 2003, The Seventh Report of The Joint National Commitee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure, JAMA; 289: 2560. Claesson, L., Gosman-Hedstrom, G., Johannesson, M., Fagerberg, B.,
Damayanti, T., 2010, Analisis Biaya Terapi Pasien Stroke Rawat Inap di RSUP Dr. Sardjito Yogyakarta Tahun 2007, Tesis, Universitas Gadjah Mada, Yogyakarta.
Dean, W., Margenthaler, J., 1990, Piracetam (Nootropyl), Smart Drug & Nutrient, [Online], http://piracetam&citicoline/CERI_PiracetamChaper from_i_ smart drug & nutrients, {2013, Januari 5].
Deutsch, A., Granger, C. V., Heinemann, A. W., Fiedler, R. C., DeJong, G., Kane, R. L., Ottenbacher, K. J., Naughton, J. P., Trevisan, M., 2006, Poststroke Rehabilitation: Outcomes and Reimbursement of Inpatient Rehabilitation Facilities and Subacute Rehabilitation Programs, American Heart Association, Inc, [Online], http://www.strokeaha.org, [2012, April 19]. DiPiro, J.T, Talbert, R.L., Yee, G.C., Matzke, G.R., Well, B.G., Posey, L.M.,
2005. Pharmacotherapy : A Pathophysiologic Approach, Sixth Edition, 415-425, The McGraw-Hill Companies, Inc, New York.
Gupta, S. K., Gupta, A., Gondhotra, D., Gupta, A., Gupta, S., 2008, Role of Citicoline in Ishaemic Stroke, Department of Neurology and G Medicine, Govt, Medical College Jammu-J&K, India, Vol 10 no 4, Otober-December 2008, 160-162.
Harsono, E.D., 2000, Kapita Selekta Neurologi, Ed.2, Gadjah Mada University Press, Yogyakarta, 81.
Hendratini, 2007, Alternatif Pembayaran Provider dalam Asuransi Kesehatan, [Online], http://www.aihhw.gov.au, [2012, April 19].
Hill M.D, Yiannakoulias N, Jeerakathil T, Tu J.V, Svenson L.W, Schopflocher D.P, The high risk of stroke immediately after transient ischemic attack, 2004, Neurology, 62:2015-2020, American Academy of Neurology.
Harrison’s Manual of Medicine, 16th ed, McGraw-Hill, Medical Publishing Division, New York.
Koda-Kimble M.A., Young L.Y., Kradjan W.A., Guglielmo B.J., 2005, Applied Therapeutics : The Clinical Use of Drugs, 8th ed, Lippincott Williams and Wilkin, Philadelphia.
Kristensen, B., Malm, J., Nilsson, T. K., Huitdin, J., Carlberg, B., Dahlen, G., Olsson, T., 1999, Hyperhomocysteinemia and Hypofibrinolysis in Young Adults with Ischemic Stroke, Stroke. 30: 974-980.
Laksmiasanti L, Harsono, Sugianto, Widyo K, Kumpulan Makalah Seminar Stroke IVIII, Mei 2003, RS Bethesda, Yogyakarta.
Lumbantobing SM, 2003, Stroke Bencana Peredaran Darah di Otak, Fakultas Kedokteran Universitas Indonesia, Jakarta.
Mayberg MR, Chair; H, Batjer H, Dacey R, Diringer M, Haley E.C, Heros R.C, Sternau L.L, Torner J, Adams H.P.Jr, Feinberg W, Thies W; 1994, Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage, Americans Heart Association, 71-0060.
Misbach J, Tobing S.M.L., Ranakusuma T.A.S., Suryamiharja A, Harris S, Bustami M, 2007, Guideline Stroke 2007 (Edisi Revisi), Kelompok Studi Stroke Perhimpunan Dokter Spesialis Saraf Indonesia, PERDOSSI, Jakarta Mulyadi, 2005, Akuntansi Biaya, edisi V, UPP AMP YKPN, Yogyakarta.
Phillips, C., [2001], What is cost effectiveness?, [Online], http://www.evidence based medicine.co.uk, [2012, April 19].
Reeder, C. E., 1995, Overview of Pharmacoeconomics and Pharmaceutical Outcomes Evaluations, American Journal of Health-System Pharmacy, ASHP, 330(3): 679-686.
Sugiyanto, K.C., 2009, Analisis Biaya Pengobatan Stroke Iskemik Sebagai Pertimbangan Dalam Penetapan Pembiayaan Kesehatan Berdasar INA-DRGs di RSUP Dr. Sardjito, Tesis, Universitas Gadjah Mada, Yogyakarta. Sulastomo, 2007, Manajemen Kesehatan, 21-24, PT. Gramedia Pustaka Utama,
Jakarta.
Tan, N. C., Venketasubramanian, N., Saw, S. M., Tjia, H. T., 2002, Hyperhomocysteinemia and Risk of Ischemic Stroke Among Young Asian Adults, Stroke. 33: 1956-1962.
The European Stroke Initiative Executive Commitee and the EUSI Writing Commitee, 2003, European Stroke Initiative Recommendations for Stroke Management-Update 2003, Cerebrovasc. Dis., 16:311-337.
Vinks T.H., deKoning F.H., deLange T.M., Egberts T.C., Identification of Potential Drug-related Problems in the Elderly : The Role of the Community Pharmacists, 2006, Pharm World. Sci, 28(1):33-38.
Vogenberg, F.R., 2001, Introduction to Applied Pharmacoeconomics, McGraw-Hill, New York.
Walley, T., 2004, Pharmacoeconomics, Churchill Livingstone Press, Philadelphia, 102-125.