Diagnostic
Accuracy of
Frozen
Section
in
Various
Thyroid
Disorders
as
Compared
with
Paraffin
Section
from
the
Same
Cases
Kuntjoro,
Benyamin Makes
Abstrak
Penelitian ini adalah pettelitian retrospektif yang nenggunakan data
dari
Sub Unit Patologi Anatottti, Instalasi Bedah Sentral, RS Dr-CiptoMangunkusuno,nulaiJanuarilggosanpaiDesetnberlggl.Selannduatahundilakukan20Tkasuspotongbekujaringantiroid' Dari
185 kasus yang diteliti,ditet,tukan 157 kasus (84,9%) kelainan jinak dan28
kasus (15,1%) ganas. pada sediaan parafinditenukan 158 kasus (85,4%) jinakdan 27 (14,8%) ganas. Terdapat positif palsu 3 kasus dannegatif patsi 2 kasus- Sensitivitas ntencapai 92,6%, spesifisitas 98,1%, ketepatan keseluruhan 97,3%, nilai ratnalan positif 89,3% dan nilai ratnalan negatif 9g,7%. Dengan analisis tersebut disimpulkan bahwa ketepatan diagnosis potong bekujaringan tiroid cukup tinggi, sehingga cara
ini
tnasih diperiukan dalatn nenentukan kcganasan tiroid dengan cepat.Abstract
(This is a retrospective study using the
datafron
the Anatotttic Pathology SubIlnit of the Central
Surgerl, Instalationof
theDr'
Cipto Mangunkusunn Hospital,frou
Januari 1990 to Decetnber 1991. During ot*o-y"o,
p"riod there were 207 cases of thyroid frozen sectiotts. A ttuuberof
185 cases have been reviewed, 157 (84.g%) were benignind Zt
(15.1%) were nnlignant. Inparafin
sectiotts 158 cases (85.4%) were benign and 27 cases (14.6%) were tnalignatû. There were 3
false positive and 2 false negatiie cases. The sensitivity was 92.6%,
specificirl'
98.1% and the accuracy 97.3%. The positive predictive i,alue was g9.3% and the negative predictive value 98.7To.Fron
the analT'5i5 we conclude that there is high accuracy infrozen section diagnosis of the thyroid nùules.This ttrethod is still necessary to decide rapidly any thrroid nalignancy.
Keywords: accurac),, th!roid froZen sectio1.
INTRODUCTION
The major
reasonfor performing
frozen section
is to
obtain
adiagnosis
of
apathologic
process,chiefl,y
todetermine
quickly whether
it
is malignant
or
benign.Another
reason is todetermine
the presence or absenceof tumor
metastasisin lymph
nodes. Frozen sectionis
also done for tissue identification
and for
determina-tion of the
adequacyof
resection margins of
a malig-nant lesion.In
otherwords,
frozen sectionwill
help the surgeon todetermine
thetreatment.
Since diagnosis ismade by the
pathologist,
the resultof
the frozen sectionwill
have serious consequencesin
the treatmentof
thepatient. So, the accuracy
of
this
method
has
to
beevaluated.
In
general,
frozen
section has a high
degreeof
accuracy.'
" Forthyroid
tissue, the accuracy isclaimed
to
be
about 87% to nearly 9TTo!-to We hope that
asurgeon can determine and
take the
right
tissue
samples.No pathologist
canovercome
the handicapof
choosing
the inaccurate tissue.Consequently,
both thesurgeon and the pathologist
needto understand
eachother to
give maximum
services.t'6'll
The
useof this
technique
is
limited
and the evaluation
is
more
dif-slid
itess.T
ty in frozen section is in
d
y
on
follicular
lesions.
We
ndiagnosing
thenodule.
So,
nand we
don't find vascular or capsular invasion, we
must delay the diagnosis,
till
the paraffin slide in
processis
ready to use.The
aim of
this retrospective study
is toknow
the accuracyof
frozen section diagnosis in
some54
Kuntjoro and Makesdisorders compared
with
paraffin section
from
the same cases,MATERIALS
AND METHODS
The
material
wasobtained
from
theAnatomic
Pathol-ogy
SubUnit of
theCentral
SurgeryInstalation
of
theCipto
Mangunkusumo
I{ospital from
January
1990 toDesember 1991.
All
their clinical
data and
paraffin
sections were examined.
We found
anumber
of
2O7 casesof thyroid
frozen
sectionswithin
theperiod
and185
of
which were included
in
this
research. The
remainder were
not
included
in
this
research becausethe slides were
lost (4
cases) andthe rest were
caseswith follicular
lesions
(18 cases).Efficacy
To
evaluate the accuracy
of frozen
section
diagnosis we need toknow
theefficacy of
this method.Therefore
we
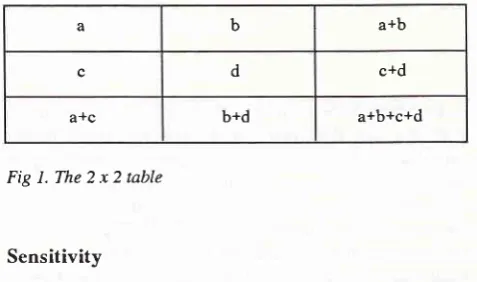
madebinomial
random numbers to simulate
the 2x
2table
asshown
in Fig
1.Efficacy
is theproporsion
of
malignancy
coinciding with paraftin
diagnosis
as agold
standard. Comparison between
this
method
andthe
gold
standardproduces
4 possibilities,
those
are: truepositive
(a), falsepositive
(b), true negative d) and falsenegative
(c).Fig
l.The2x2table
Sensitivity
Sensitivity
is
theprobability
that
themalignant tumor
can be
diagnosed
on the patients proved
to
bear
amalignant tumor.
true positive
Sensitivity
=true
positive
+false negative
Type of lesionMed J Indones
Accuracy
Accuracy
is
specificity.
Accuracy =
the combination
of
sensitivity
and
true positive + true negative
true Pos. + false Pos. + true neg. + false neg.
Positive and
negative
predictive value
Positive predictive
valueof
a test is theprobability
that apatient
has amalignant
tumor
if
the test is
positive
for
malignant tumor.
true positive Positive predictive value =
true positive + false positive
Negative
predictive value of a
test
is
the
probability
that a patient
has
no malignant tumor
if
the test
is
negative.true negative Negative predictive value =
true negative + false negative
RESULTS
From the
185 casesstudied
wefound I57
(84.9%)
and28 (15.1%)
caseswith benign
and
malignant
lesionsrespectively,
at frozen
section.
Benign
lesions cover
adenomatous
goiter,
Basedow's disease, chronic
thyroiditis
and thyroglossal
cyst
(seeTable
1),while
malignant lesions consist
of papillary
carcinoma,
fol-licular
carcinoma, anaplastic carcinoma and
uniden-tified
carcinoma
(seeTable
2).Table
l.
Benign lesions at frozen sectionnumber of cases
%
Specificity
Specificity is
the
probability
that
abenign lesion
can be diagnosed onpatients having no malignant tumor.
true
negative
Adenomatous goiter Basedow's disease
Chronic thyroiditis Thyroglossal cyst
r53 2
I
I
97.5
1.3 0.6 0.6
a b a+b
c d c+d
a+c b+d a+b+c+d
Specificity
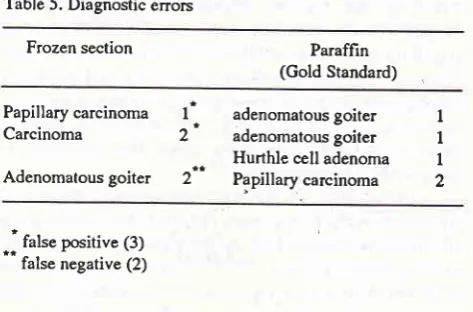
= [image:2.595.45.284.425.566.2]Table 2. Malignant lesions at frozen section Table 5. Diagnostic errors
Frozen section Paraffin (Gold Standard)
Type of lesion number of cases
%
Papillary carcinoma Follicular carcinoma Anaplastic carcinoma Carcinoma
Papillary
carcinoma
lt
Carcinoma
2'
Adenomatous
goiter 2"
adenomatous
goiter
I
adenomatous
goiter
I
Hurthle cell
adenoma
I
PSnillaV
carcinoma
216
5 3
4
57.
I
t7.9 to.7
14.3
Total
From
paraffin
sections there
were
158benign and27
malignant lesion
cases.
Benign lesions
cover
adenomatous
goiter, follicular
adenoma,Hurthle cell
adenoma,Basedow's
disease,chronic thyroiditis
andthyroglossal cyst (Table 3). Malignant
lesions cover
papillary
carcinoma,
follicular
carcinoma,
anaplasticcarcinoma,
Hurthle cell
carcinoma
and squamouscell
carcinoma
(seeTable
4).Table 3. Benign lesions at paraffin section
*'
fulr" positive (3)false negative (2)
From
the above datawe found
three falsepositive
andtwo
false negative
cases(see
Table 5).
After
being
analysed
we
found that the sensitivity was
92.6%, specificity
9L l
7o, accuracy9i
.3 %,pos it ivepredictive
value
89.3Vo andnegative
predictive
value98.7%.
DISCUSSION
Thyroid
frozen section
needschoosing
the samplein
detail, both by
surgeon
andpathologist. The
wrong
sample makes false negative.o
Macroscopic examination
is
necessary.
At
macroscopic examination
we areusually
ableto
makean
estimation of
the diagnosis.For
the exact diagnosis,we
need
histopathological examination.
To
increasethe accuracy
of
frozen
section
needsother
examina-tions,
for
example,
fine
needle aspiration
andimprint
cytology, Aspiration
andimprint cytology's
cells
canbe observed
clearly by both
cytologic
examinations.
It
is
said that
imprint cytology
can help
to
increase the accuracyof
frozen section
diagnosis.2, l2't3.t4,t5In
this
observation
we get
97.3Voof accuracy.
There
aresome
different
results
from other
observa-tions, ranging
from
87
lonearly
98To.The most common benign lesion is
adenomatousgoiter. The histological picture
of
this lesion
varies.There
are large andsmall
follicles.
The large
follicles
arelined by flat epithelium
andthe lumen
filled with
colloid.
The
small
follicles
are
lined
by
thora-cal/cuboidal epithelial cells, the lumen
is
empty or
filled with
asmall
amountof
colloid.
Usually
there arefibrosis,
haemorrhages andcalcifications.
Sometimesit is
encapsulated and
difficult
to
differentiate from
follicular
adenoma.6' 16, l7The
most common
thyroid
malignancy is
papil-lary carcinoma. This
lesion
is markedby
the presenceof
papillary
growth,
psammoma bodies and nuclear
changes,
The
nuclear chromatin groups
at
the
periphery
of
the nucleus and has
a
ground glass
ap-pearanceor orphan Annie
nuclei.6'1618,19whereas
at100
Type of lesion
,'/
number
of cases 7oAdenomatous goiter Follicular adenoma
Hurthle cell adenoma
Basedow's disease
Chronic thyroiditis Thyroglossal cyst
150 2 2
2
I
I
94.9 1.3 1.3 1.3
0.6 0.6
Total 158 100
Table 4. Malignant lesions at paraffin section
Type of lesion number of cases
%
Papillary carcinoma Follicular carcinoma Anaplastic carcinoma Hurthle cell carcinoma
Squamous cell carcinoma
19 5
I
I
I
70.4
18.5 3.7 3.7 3.7
[image:3.595.296.533.93.249.2] [image:3.595.36.270.106.243.2] [image:3.595.33.268.244.760.2]56
Kuntjoro and Makescytology,
we
can see intranuclear cytoplasmic
in-vâginuiion"
in
papillary
carcinoma.6'[o't8'zo
Not
all
papillary growth
is
malignant. There are
some
dif-ferences between
papillary carcinoma
and
papillary
hyperplasia.
In papillary
hyperplasia the
cells
arear-ranged
as
one layer
and the
round nuclei lay at
thebasal
or at
the
middle
of
the
cells.
The
chromatin
isdelicate and homoge.ro*.6'
16In this
study,
follicular
carcinoma
is
diagnosedby frozen section
in
5 cases(17,9%). The malignancy
of
this tumor
is
marked
by
the existence
of
vascularand capsular
invasion.ll
't6't1'21Follicular
carcinoma
is
devided
into two
types,
those
are minimally
andwidely
invasive.
Forpathologist,
the maindifficulty
isin
distinguishing
minimally
invasive
follicular
car-cinoma from
follicular
adenoma
for
the two
lesionshave the same appearance both in histological I l'16'17'19
and
cytological
picture.6'15'17 The maligriancy isdeter-mined by the
existence
of
capsular and vascular
in-vasion.
If the capsular and vascular invasion can not
be
found,
the diagnosis must be delayeduntil paraffin
slides are
prepared
and this lesion
is
grouped
into
follicular
lesion.oFrom paraffin section,
these
follicular
lesionsconsist of adenomatous
goitre,
follicular
adenoma,fol-licular carcinoma and
follicular
variant
of
papillary
carcinoma,6
In widely
invasive
thyroid
carcinoma, the
tumor
cells
have invaded the
blood
vesselsor
spreadout
of
thecapsul so that, there is
no
problem
in making
the diagnosis.In
this
study there were
3 cases
(10,77o)
of
anaplastic
carcinoma diagnosed by frozen section.
The
diagnosis
of
this type
of
malignancy
is
basedon
theexistence
of
cell
anaplasia,
without
folicle formation
and the existence
of
necrosis.The tumor cells
vary in
diametres.
They
can be
small with
round
nuclei
andlook
like
malignant
lymphoma
cells,
spindle
shapedand
look like fibroblast or
large and multi-nucleated
(giant cells).6'l
I' 16' leThis
tumor
can be dif,ferentiatedfrom
medullary
thyroid
carcinoma,
becausethe
latter produces some
polypeptides and
factors, e.g.: calcitonin,
car-cinoembryonic antigen,
ACTH,
serotonin,
enolase't'l-'t< '
etc.--
-"
CONCLUSION
As a conclusion,
the
frozen
section diagnosis
of
thethyroid
disorders
in Dr.
Cipto Mangunkusumo
Hospi-tal
has ahigh accuracy and the
level
of
accuracy is thesame
as the
paraffin
section diagnosis.
Thus,
frozen
section
of
the
thyroid
is
still necessary
to
support
surgeon
in
making diagnosis
quickly.
Med J Indones
REFERENCES
l.
KaufmanZ,Lew
S,Griffel B,
DinbarA.
Frozen section diagnosis in surgical pathology.A
prospective analysisof
526 frozen sections. Cancer I 986;57 :3'l 7 -9.
2. Oneson
RH, Minke
IA,
Silverberg SG. Intraoperative pathologic consultation. An auditof
1,000 recentconsecu-tive cases. Am J Surg Pathol 1989;13;237-43.
3. Sawady
f,
Berner JJ, Siegler EE. Accuracy of and reasonsfor frozen sections: a corelative, retrospective study. Human pathology 1988; 19: l0 l9-23.
4. Tjahjadi G, Soutrisno E. Peranan pemeriksaan potong beku pada diagnosis keganasan. Muktamar Nasional ke-II Per-himpunan
Ahli
Bedah Tumor Indonesia. Iakarta, 7-9 April1983.
5.
Taufik E,
MangunkusumoR.
Peran potong beku pada penanganan tumor ovarium, In:Kumpulan naskah lengkap Kongres Nasional ke X IAPL Surabaya, 5-8 Juli 1990.6. Kraemer
BB.
Thyroid.In:Silva EG, Kraemet BB (editor) Intraoperative pathologic diagnosis frozen section and other techniques. Sydney: William & Walkins, 1987:51-69.7. Shaha
A,
GleichL,
Di
Maio T, JaffeBM.
Accuracy andpitfalls
of
frozen section during thyroid surgery.I
SurgOncol 1990; 44:84-92.
8. Irish
IC,
van Nostrand AWP, Asa SL, Gullane P, Rotstein L. Accuracy of pathologic diagnosis in thyroid lesions. Arch Otolaryngol Head Neck Surg 1992;118:918-22.9. Rosen
Y,
RosenblattP,
SaltzmanE.
Intraoperativepathologic diagnosis
of
the thyroid neoplasms. Report on experience with 504 specimens. Cancer 1990;66:2001-6.10. Kingston GW, Bugis SP, Davis
N.
Role of frozen section and clinical parameters in distinguishing benign fiom malig-nant folicular neoplasms of the thyroid. Am J Surg 1992; 164: 6O3-5.11. Mendelsohn G. Pathology of the thyroid disease. In:
Diag-nosis and pathology ofthe endocrine disease. Philadelphia: Lippincott, 1988:37-1 17.
12. Pluot
M,
FarouxMI,
PateyM,
MallaisyT,
Simatos A.Contributions of imprint cytology to the diagnosis of tumots of the thyroid. Arch Anat Cytol Path 1989;37:36-9.
13. Abrahams C. The scrimp tecnique-a methode for the rapid diagnosis of surgical pathology specimens. Histopathology 1979;2:255-66.
14. Kontozoglou TE, Cramer
HM.
The advantagesof
in-traoperative cytology. Analysis of 215 smears and review of
the literature. Acta cytologica 1991;35:154-64.
15. Mair S, Lash RH, Suskin D, Mendelshon G. Intraoperative
surgical specimen evaluation: frozen section analysis,
cytologic examination, or both? A comparative study of 206 cases. Am J Clin Pathol
l99l;96:8-14.
16.
Lloyd RV. Thyroid.
In:Endocrine pathology. New York:Springer-Verla g, L99 O:37 -69.
17. LiVolsi
VA.
Follicular lesions of the thyroid. In: Surgical pathology of the thyroid. Philadelphia: WB Saunders, 1990:173-2t2.
19. Hedinger C, Williams ED, Sobin LH. Histological typing of tumours. 2nd ed. Berlin: Springer-Verlag, 1988.
20.
Orell
SR,
Sterrett GF, WaltersMNI,
WhitakerD. The
thyroid gland. In: lvlanual and atlas of hne needle aspiration cytology. Edinburgh: Churchill Livingsrone, 1986:65-86.2I.
Rosai J, Carcangiu ML, De Lellis RA. Tumors of the thyroid gland.Atlas
of
tumor
pathology. 3rd ser. Washington DC:AFIP, 199O:49-63.22.
Lloyd RV,
Sisson JC, MarangospJ. Calcitonin,
car-cinoembryonic antigen and neuron-specific enolase in medullarythyroid câlcnoma.
An
immunohistochemical study. Cancer 1983 ;5 I :2234-9.23. Birkenhager JC, Upton
GV, Seldentarh
HJ, Krieger DT, TashjianJr AH.
Medullary thyroid
carcinoma:ectopic productionof
peptideswith
ACTH-like, corticotrophin
releasing factorlike and prolactin production-stimulating
ac-tivities. Acta Endocrinol 1976;83:280-92.
24. Deflos LJ, Bone
III
HG, Parthemore IG.Immunohistologi-cal studies of medullary thyroid carcinoma and C cell hyper-plasia. J Clin Endocrinol Metab 1980;51:857-62.