VoL 8, No 2, April - June 1999 Clinicopathology and risk
factors
in breast cancer
123Clinicopathology
profTle
evaluated against
several
risk factors
in breast cancer
cases
Idral Darwis*, Muchlis Ramli*, Didid Tjindarbumi*, Esti Soetrisno#,Gunawan
Tjahjadi#, Endang
Sri
Roostini#, Santoso Cornain#,
Drupadi
SDillon-,
JoedoPrihartono$, Setyawati
Budiningsihs, Goi Sakamoto'
Yoshiyuki Ohno', Kenji Wakair
Abstrak
Telah dilakt'tkan penelitian dua ratus dua puluh enam kasus kanker payudara (KPD) yang berhubungan dengan aspek klinik dan patologi serta faktor risiko yang berhubungatt dengan terjadinya keganasan payudara. Distribusi terbanyak pada umur antara 35-55 tahun clengan frekuensi tertinggi antara umur 40-50 tahun. Tidak didapatkan perbednan lokasi tumor pada payudara kanan atau kiri serta distribusi pre-menopause maupun post-menopause. Delapan puluh satu koma enarn persen KPD ditemukan pada stadium lanjut (stacliutn
IIIA:
17,77o, IIIB: 56,2Vo dan IV: I l,9Ea), sedangkan stadium I: I,3Vo dan stadiumII:
ll,97o. Tujuh puluh tima dari 226 kasus dilakukan tindakan pembedalnn: 60Vo mastektomi simpel, 26,7Vo mastektomi radikaL dan l,3Vo: breast concerving treatment (BCT). His-topatol.ogi dari jaringan payudara dari 2I4 kasus clklapatkan karsinoma int,astf yang terdiri dari: 90,47o karsinoma eluktal invasif dan 9,6Vo tipe khusus. Dilakukan analisa dari beberapafaktor risiko seperti status kawin, umur pada saat kawin pertama, untur menarche, sttttus menoPause, laktasi, riwayat keluarga KPD, penggunaan kontrasepsi dan konsumsi tinggi lemak. Hasil dari metode kasuskontol
ntenunjukkan bahwa faktor-faktor status menopause, laktasi dan konsumsi tinggi lemak meningkatkut risiko terjadinya KPD, dengan risiko relatif ntasing-rnasing: 1,5 1, I,83 dan2,6l.Abstract
The second batch case-controL study on breast cancer hcts been conducted as a joint study between Indonesian antl Japan. Two hwrdrerl antl hventy six (226) cases of breast cancer was coLlected to assess the riskfactors ancl evaluatetl
for
their clinical presentation of the clisease. The age distribution in some high risk areas showed at age 35 to 55 years, with a single peak between 40 to 50. There was no dffirence in nuntber of cases in respect to tu,nor site anel menopausal status. The majority of cases 81.6 Vo were in advanced stage (lllA: 17.7%, IIIB: 56.2Vo and IV: Il.9Vo) whiLe in contrast stage I and II were very rare (I.3Vo and ]l.9Vo respectively). OnLy 75 cases were operabLe; simple masîectomy was the most frequent sur7ery carried out (60.0Vo), followed by moclffied radical mastectomy (26.7Vo), classical radical mastectomy ( 12Vo) ancl breast consenting treatnrcnt ( I .3Vo). The specimens were reviewecl using classification reconntentletl by the Japanese Breast Cancer Society reveaLecl invasive ductaL carcinoma (90.4 Vo) and the special type (9.6 Vo). Several riskfactors were analyzedfor their influence to the deveLopment of breast cance4 narnely: marital status, ageatrtr$
marriage, menarche, menoltattsaL status, lactation, fLtmily history of breas't canceq, use of contraceptive ancl fat consLuryttion. Among the characteristics studied, tltefoLlowingfactorssignificantlyincreasedtheriskof breastca.ncer:menopausaLsturus(RR=1.51:95VoCI:1.10-2.09),non-lackLting children(RR=1.83;95VoCI:1.07-3.11)arulfatconsuntption(RR=2.61;95VoCI:1.86-3.68),whiletheuseofcontraceptiveshoweclpro-tective effect. The fi,ndings wilL be discr.tssed in its benef.t relative to both the improvement of tlxe treament modality ancl the cancer controlP roSranx.
Keywords: Breast cance6 clinicopathologicaL, case-controL study, epidemiology
*
Department of Surgery, Facuhy of Medicine, Universityof
Inelonesia, Jakarta I 04 30, I ndo nesia#
Deparment of Pathology, FctcuLty of Medicine, Universityof
Indones ia, Jakarta I 04 30, Indonesia*
Department of Nutitiort, FacuLty of Medicine, Liniversityof
Indonesia, J akarta I 0430, Indonesia
*
Department of Community Medicine, Faculty of Medicine, University of Indonesia, Jakarta 10320, Indonesia.
Department of Pathology, Cancer Institute Hospitctl, Tbkyo 170, Japant
Deparment of Prettenth,e Medicine, SchooL of Medicine, Nagoya University, Nagoya 466, JapanINTRODUCTION
Carcinoma of
the breast
continue
to
baffle the
sur-geons
and the pathologists
for
the unpredictable
bio-logical behavior and many gap
in
the knowledge
of
the factors
that either control
or
influence tumor
genesis and growth.
In
Indonesia breast
cancer
ranked
secondmost
common malignant tumor of
theStand-Darwis et
al
ardize
Cancer Ratio (ASCAP.)
17.84Vo 18.44Vo(ASCAR
I7.48Vo)
in
1989.r1988
andMore articles
have
beenpublished
onbreast
cancer'2' 7but accumulation
of
knowledge
hasnot produce
anycommensurate degree
of
agreement among
researchworker
andclinicians
onepidemiological, etiological,
pathological
and treatment
problem
of
breast cancer.
Thomas Huxley wrote
"A
great
tragedy
of science
-the staying
of
abeautiful
hypothesis
by
anugly fact".
Wider understanding
of
different modalities,
natural
history
of
the
disease andhost-tumor relationship
aresome
of
the encouraging factors toward better
sal-vage of
this
disease.A
team work is
neededfor
themanagement
of
breastcancer
without
prejudice to
thespecialty.
This
study was conducted
to
find
out the
clinico-pathological findings
and
incidence of the
diseasein
relation to
other
parametersalong
with
theknown
eti-ological
factors.
MATERIAL
AND METHODS
Materials
consisted
of
women who
underwent
treat-ment at
the
Division
of
Surgical Oncology,
Depart-ment
of Surgery
-
Dr. Cipto Mangunkusumo
Hospi-tal,
Jakarta, during the period
of
February
7992
to
September
1995 and
were
diagnosed as
having
his-tologically confirmed
breast carcinoma.
The
medical
records
comprising
226
cases,aged
29
to
74 years
(median
age
45
years),
were reviewed.
A
detailed
clinical history
and
clinical examination
were taken.
Clinical
staging was done
by criteria
according to
theInternational
UICC
TNM
System
for Malignant
Tu-mor8 andthe surgical
specimenswere reviewed using
the
classification
recommended
by
the
JapaneseBreast Cancer
Society
(1984)e.With
the
same
cases(226) several
potential
factors
for
breast
carcinoma, namely: marital
status, age at
first
marriage, menarche,
menopausal status,
lacta-tion,
family
history
of
breast cancer, use
of
contra-ceptive
and fat
consumption were
recorded.
A
case-control
study design with
1:2ratio
was applied
in
this
assessment.
Each
risk
factor
was
assessedthrough
univariate analysis and was
measured
its estimated
Relative
Risk
and 95Vo
Confidence Intervals.
RESULTS
Age
We found that
signif,rcant increase
of
the proportion
Med
J
Inclonesof breast cancer
casesin
women
started and
peaked atcomparatively
younger
age as comparedto
women
in
the Western countries.
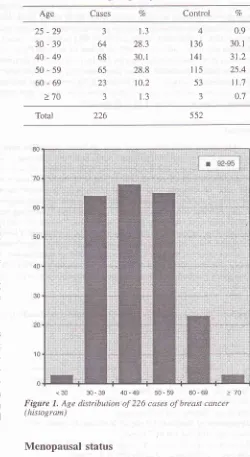
Table
1 andFigurel
showsthe details
of
ageincidence and the commonest
inci-dence was
in
age groups 30-39,
40-49
and
50-59
(28.3Vo, 30.1Vo
and
28.8Vo)
respectively.
The
inci-dence sharply
decrease
with
advancing age.
The
youngest
caseof breast
cancer
was29
years
old
andthe oldest
74
years.
Thble
1.
Distribution of 226 cases of breast cancer and 552 con-trols according to age of patientsCases % Control Vo
Age
25-29
30-39
40-49
50-59
60-69
>70
J
64
68 65 23
3
1.3
28.3
30.
l
28.810,2
1.3
4
t36
141 115 53
3
0.9
30. r 31.2
25.4
11.7
0;7
Total 226 552
[image:2.595.322.572.232.689.2]<30 30-39 40-49 50-59 60-69 >70 Figure 1, Age distribution of 226 cases of breast cancer (histogram)
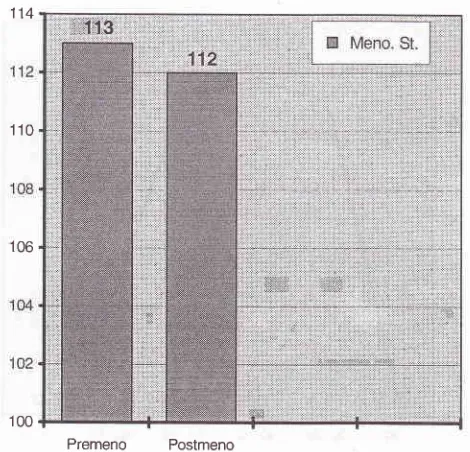
Menopausal status
Correlation with hormonal
status is shown
in
Figure
2.
One hundred thirteen
(50.22Vo) cases
were
Vol 8, No 2, April
-
June 1999 Clinicopathology ancl riskfactors
in breast cancer
125TFeatment
The treatment
modality
in operable
cases (33.2Vo)in
shown
in
Table
4. Radical
mastectomy and
modified
radical
mastectomy were adopted
asinitial
treatment
in
the Department
of
Surgery
for
StageI
and StageII
which
was done
in
29
cases.Adjuvant radiation
wasperformed
if
there
was
clinical
evidence
of
regional
metastasis. Stage
IIIA
cases
were treated
by
simple
mastectomy
(60Vo).Thble
4. Type of operation performed in 75
casesType of operation No. of cases 7o 114
110
106
1:irit!1i1,3
100
Radical mastectomy Modifi ed radical mastectomy Simple mastectomy
Lumpectomy
9
20
45
I
l2.o
26.7 60.0
1.3
[image:3.595.77.312.89.315.2]Premeno
PostmenoFigure 2, Distributiott of 225 breast cancer by menopausaL status
Clinical
features
The right
breast was
involved
in
48.2Vo,left
breastin
48.'lVo and
bilateral tumor
was presentin
1.87o(Table
2). Staging
of
the
disease(Table
3)
was done
by
rheUICC
TNM
Classification of Malignant Tumors
cri-terta:,
l.3Vo were
in
stageI, ll.9Vo
in
stageII,
17 .7Voin
stageIIIA,
56.20/oin
stageIIIB
and 11.97a in
stageIV.
The highest number
of
caseshad
advanced
dis-ease
(Stage
IIIB)
and proposed treatment was
pallia-tron.
Table
2.
Side involvement of breast cancer casesSide affected No. of cases
Histopathology
Histology classification
of
Japanese
Breast
Cancer
Society have
been adopted
to
classify breast
carci-noma (Table 5). Scirrhous
adenocarcinoma
was
thecommonest
type of
cancer.Table
5.
Histological pâttern of breast cancer cases according to classification recommended by Japanese Breast Cancer Society (1984)Histological types No. of cases Right
Left
%oVo Right
Left
Bilateral
109
lr0
4
48.2 48.7
1.8
l5
65
ll8
5
I
ll
7
27
61
4
5
2 Non-invasive carcinoma
Invasive carcinoma
a. Invasive ductal carcinoma
al.
Papillotubular a2. Solid-tubular a3. Scirrhousb. Special types
bl. Mucinous carcinoma
b4. Squamous cell carcinoma
c. Unclassified and other
8
38 57
Thble
3.
Distribution ol'breast cancer cases according to clinical staging (n = 226)Stage Cases b2, Medullary
carcinoma
l0
b3. Invasive lobular
carcinoma
5Va
I
5
3
I
I
II
IIIA
IIIB IV
Unknown
3
27 40 t27 27
2
1.3
I1.9
17.7
56.2
11.9
0.8
Total 226 100.0
Notes:
four
cases bilateral126
Darwis et aLTable
6.
Univariate logistic analySisof
odds ratios (RR) and confidence interval (CI) for breast cancer risk factorsCovariates
Cases
ControlsRR
957o ClMetl
J
IndonesMenarche <15
>
t5Menopausal status
No Yes Marital status
Married Widowed Unmarried
Use of contraception No
Yes Lactation
Yes No
Family BC No Yes
1.00
Referencer.r3
(0.82-1.56)1.00
Reference1.5r
(1.r0-2.09)*1.00
Reference0.4
(0.62-t.40)1.00
Reference0.67
(0.46-0.98)*1.00
Reference1.83
(1.07-3.il)'k1.00
Retèrence0.50
(0.22-1.3s)1.00
Reference0.81
(0.59-1.12)1.00
Reference2.61
( 1 .86-3.68)*1.00
Referencet.28
(0.93-1.'7'1)Age of marriage
)
20yrs
98< 20
yrs
121Fat consumpt <26
>26
Calories intake
<
1854
I 15>
1854
ll1
DISCUSSION
Although the
risk of
breast cancer increases with
progressing
age,2-4a
special age curve distribution
has been observed.
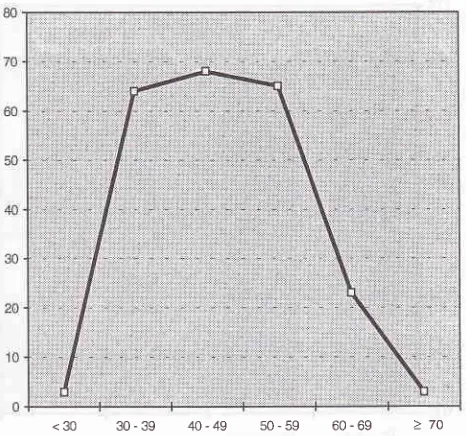
From 226
cases(Fig:
3),
breastcancer
incidence rises quickly
between ages
30
and35,
andlevels on
andoff to
aplateau between 35
and55,
and
after
age55 decline slowly. This is different
from
De Waard's
report
(1964)
of
double
peaks at 45to 49
and 65
to
70. Henningsen (1975) reported
only
single peak between 50
and 60.4Other
dissimilar
fig-ure was
incidence of
breast cancer
in young
women,
defined
as40
yearsor
less.Commission
onCarcer
of
the American College
of
Surgeons
reporled
23.974
cases
diagnosed
in
1990:
0.87owere 30
years
of
ageor
less
and6.6Vowere
in
the
age rangeof
31to 40.
In
the present
study
l.3Vowere
less30 years
and28.3Voin
the
agerange
of
30
to
39
years.s [image:4.595.347.580.95.313.2]<30 30-39 40-49 50-59
60-69Figure 3. Age distribulion curve
for
226 breast cancer patientsThe majority
(85.87a)
of
226
breast
cancer were
in
advanced
stage(
IIIA, IIIB
and
IV)
and l3.2Vo
were
in
early
stage.
The
present
study
were similar with
previous
data
but different from
breast cancer
in
Ja-pan,8-e
which the majority were
in
early
stage.
Only
on 75
casesperformed surgery and Simple
mastec-tomy
(60Vo)
was
mostly
chosen procedure due to
high portion
of
advanced stage
(IIIA).
Surgical
mo-dality
in
early
caseswere
radical
mastectomy
(l2Vo)
and
modified radical
mastectomy
(26.7Vo).Ductal
(scinhous),
solid-tubular,
papillotubular,
medullary,
mucinous and
invasive lobular
carcinoma
were diagnosed
in
52.44Vo, 28.89Vo, 6.6Vo,
4.4Vo,2.2Vo and 2.2Vo
of
cases,respectively. Consideration
of
the
histological
parameter, such
as degreeof
tubu-lar, gland
formation,
sizeof cells
andnuclei
( nuclear
pleomorphism),
degreeof hyperchromatine
andnum-ber
of
mitoses
was
also evaluated
for
prognostic
evaluation.
Subtype
of
invasive
ductal
carcinoma
re-flect
the
degreeof differentiation
such
aswell
differ-entiated, moderate
andpoor differentiated
in
anorder
of
papillotubular carcinoma, solidtubular
carcinoma
and scirrhous carcinoma. Depending
on
a
grading
system considering the above mentioned
parameters,two third
of
the
caseswere
grade
III
and
only
small
portion
grade
I.
The prognosis
is
usually
favorable
when tubular gland formation and stromal
elastosisexist
and when
tumor mitosis
and
fibrosis
are
mini-mal (Wallgren
et
al,
1916).r09 116
lt2
113
177
45 2
t'70
49
1L)4
28
213 6
65
l6l
232
2t8
270
r80
354
97 0
3r1
133
418
J3
422 22
222 222
232
220
258
[image:4.595.86.321.112.533.2]VoL
8,
No 2,April
-
June 1999Despite
of
clinical
staging, histological
type
andgrade
of
tumor
had
a role
to
predict prognosis
of
breast
cancer.This
case control study has been conducted
to
con-firm
causal relationship
of
nine important
determi-nantfactors
for the development
breast canceramong
Indonesian women (Tâble
6).
Unlike women
in
thedeveloped countries, the Indonesian
women differ in
many
aspectssuch
asfamilial,
non familial
(environ-ments) and
socio-economically.
Nine
determinant
factors have been
assessedusing univariate
analysis
(Table
6),
andthree of them showed significant
asso-ciations
with
the
development
of
breast
cancer,namely: menopausal
status(RR=I.51:95Vo
CI:
1.10-2.09),lactation
(RR=1.83;95Vo
CI:
1.07-3.11)
andfat
consumption (RR=2
61; 95VoCI:1.86-3.68). Menarche
and the use
of
contraceptive
which
arerelated to
en-docrine factors had not been found to be significant
factor
in this study. The earlier
the
ageof
menarche,with
its
associated
earlier
onset
of
"regular"
mens-trual
cycles,
the higher
risk of
breast cancerlo. The
findings
were not consistent with
thenotion that early
menarche had been demonstrated as a risk factor in
many studies.
It
is
known that the interval from
themenarche
up
to
the establishment
of
regular
men-strual cycle might
be abetter estimate for
determinat-ing
the
risk for
breast cancer
rather than the age
of
menarche.
Women
with
early menarche
(age 12 or
younger) and rapid establishment
of
regular
cycles
had analmost
fourfold
increasedrisk of
breastcancer
when compared
with women
with
late
menarche (age 13or older)
andlong
duration of irregular cycles.l
l-12The use
of
contraceptive showed
protective effect in
this study,
which
wasdifferent from
the results of
thefirst
batch
of
study. The discrepancy
might
be dueto
small
samples.
Such unclear
findings were also
re-ported elsewhere,
thus, further study is
necessaryto
clarify
the effect.
Acknowledgments
The authors are grateful to the
nurses, Ms.
Emi
andMs. Ros and
for
Public Health Nurses,
Ms.
July
andMs.
Erlaini for
excellent
care and
collection
of
dataof
breast cancer
casesand controls. We are also
in-debtedto the laboratory technician
for excellent
work
on the surgicopathological
specimens.ClinicopathoLogy and risk
factors
in
breastcancer
127This work was supported
by the
Ministry of
Educa-tion,
Science,
Sports and Culture
of
Japanese Gov-ernment, Grants No.01M2007,MM20I3
and0ffi2CfJl6:
and
was
partly
supported
by
the Indonesian
Cancer
Foundation.
This collaborative study was a part
of
Special Cancer
ResearchProject in Monbusho
Inter-national Scientific
Research
Program,
with
the
ap-proval
of
the Dean, Faculty
of
Medicine University
of Indonesia,
No. 4383ÆT02.H4.FK/E| 88.
REFERENCES
1.
Cornain S, Mangunkusumo R, NasarIM,
Prihartono J. TenMost Frequent Cancers in Indonesia: Pathology based Can-cer Registry Data of 1988-1992. In: Cancer Registry in
Indo-nesia. National Cancer Register Center, Jakarta Coordinating
Board,1997.
2.
VorherrH.
Breast Cancer-
Epidemiology, Endocrinology, Biochemistry and Pathobiology, Urban&
Schwarzenberg,Inc., Baltimore
-
Munich, 1980:25-36.3.
Vaidya MP, Shukla HS, A Textbook of Breast Cancer, New Delhi: Vikas Publishing House PVT LTD, 1983:124-304.
Winchester DP. Breast Cancer in Young Vy'omen., TheSurgi-cal Clinic of North America,1996;76-2: 279-87
5.
Boyd NF. Epidemiology of cancer. In: Tannock IF,Hill
RP,editors. The Basic Science of Oncology, 2nd ed. Canada: Mc. Graw-Hill, Inc. 1992: 7 -21.
6.
Donn AS,Muir
CS. Breast cancer: Epidemiology and riskfactors. In: Khogali M, Omar YT, Gjorgov A, Ismail AS,
edi-tors. Cancer Prevention
in
Developing Countries. Oxford,Pergamon Press, 1986: 155-66.
7.
Kelsey JL, Horn-Ross PL. Breast cancer: Magnitude of theproblem and descriptive. Epidemiol Reviews 1993; 15: 7 -17 .
8. TNM Atlas: Illustrated Guide ro the TNM / P.TNM Classifi-cation of Malignant Tumours, 3.d ed. Berlin: UICC Springer Verlag,1990: 173-83.
9.
Japanese Breast Cancer Society, The General Rules forClini-cal and Pathological Recording of Breast Canceq Jpn J Surg
1989; 19: 612-32.
10. Apter D, Vihko R. Early menarche, a risk factor for breast
cancer, indicates early onset of ovulatory cycles. J. Clin
En-docrinol Metab 1983; 57: 82.
I 1. Henderson BE, HS Fergelson. In: Text Book of Breast
Can-cer-Clinical Guide to Therapy, United Kingdom Biddles Ltd, 1998:1-16.
12. Henderson BE, Ross RK, Judd HL, et al. Do regular
ovula-tory
cycles increase breast cancerrisk?
Cancer 1985;56:1206.
13. Kelsey JL, Gammon. The Epidemiology
of
Breast Carrcer.