SOP-Ankle Joint, ID#ARA 01, Rev 1#| 1 SOP-Ankle Joint ID#ARA 01 Rev 1# 13 Mei 2015 30 Halaman
Standar Operasional Prosedur
Permasalahan Sendi Pergelangan Kaki
SOP - Ankle & Foot ProblemsDiperuntukkan pelayanan ARA Physiotherapy UPH-Karawaci & Bodysoul-Kemang
Rev 1# 13 Mei 2015
Disusun Oleh
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 2 1. Anatomi 1.1Tulang 1.1.1 Tibia 1.1.2 Fibula 1.1.3 Talus 1.1.4 Calcaneus 1.1.5 Navicular 1.1.6 Cuboid 1.1.7 Cuneiform 1,2,3,& 4 1.1.8 Metatarsal 1,2,3,4,&5 1.1.9 Phalang1,2,3,4,&5
Gambar 1.1 Kaki kanan tampak atas
Gambar 1.2 Kaki kanan tampak bawah
Gambar 1.3 kaki kanan tampak belakang (posterior)
1.2Sendi
1.2.1 Tibiafibular joint inferior 1.2.2 Tibiotalar joint
1.2.3 Calcaneofibular joint 1.2.4 Talocalcaneal joint 1.2.5 Talofibular joint
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 3 1.3Ligamen 1.3.1 tibiofibular ligament 1.3.2 tibiotalar ligament 1.3.3 talofibular ligament 1.3.4 calcaneofibular ligament
1.3.5 posterior tibiofibular ligament 1.3.6 posterior talofibular ligament 1.3.7 posterior talocalcaneal ligament 1.3.8 deltoid ligament
Gambar 1.4 Ligamen kaki kanan sisi belakang (posterior) Gambar 1.5 Ligamen kaki kanan sisi depan
Gambar 1.6 Ligamen kaki kanan sisi lateral Gambar 1.7 Ligamen kaki kanan sisi medial Interosseous membrane Posterior tibiofibular ligament Posterior talofibular ligament calcaneofibular ligament deltoid ligament
talofibular ligament tibiotalar ligament
talofibular ligament Interosseous
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 4
Gambar 1.8 ligamen kaki kanan sisi medial Gambar 1.9 ligamen kaki kanan sisi plantar
1.4Otot
Gambar 1.10 Otot Ekstremitas bawah kanan sisi anterior
Gambar 1.11 Otot ekstensor pergelangan kaki kanan sisi anterior
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 5
Gambar 1.12 Otot ekstensor halluces longus & tibilais anterior
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 6 Gambar 1.14 Otot ekstremitas bawah sisi posterior Gambar 1.15 Otot ekstremitas bawah sisi posterior
dengan plantar fleksi (a)
Gambar 1.16 Otot ekstremitas bawah sisi posterior dengan plantar fleksi (b)
Gambar 1.17 Otot ekstremitas bawah sisi posterior dengan plantar fleksi (c)
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 7
Gambar 1.18 Tendon ekstremitas bawah sisi posterior & anterior
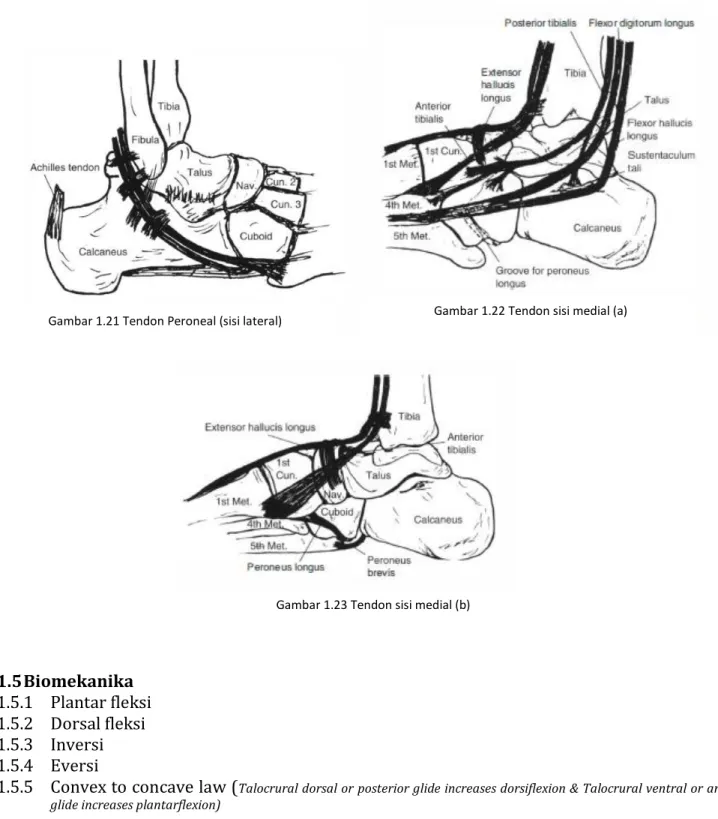
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 8 1.5Biomekanika 1.5.1 Plantar fleksi 1.5.2 Dorsal fleksi 1.5.3 Inversi 1.5.4 Eversi
1.5.5 Convex to concave law (Talocrural dorsal or posterior glide increases dorsiflexion & Talocrural ventral or anterior glide increases plantarflexion)
Gambar 1.21 Tendon Peroneal (sisi lateral) Gambar 1.22 Tendon sisi medial (a)
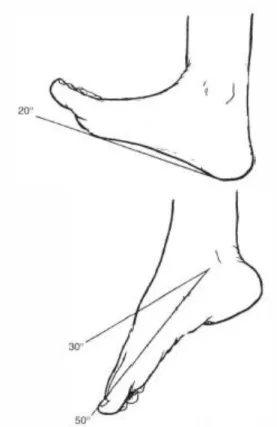
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 9 Gambar 1.24 Gerakan normal dorsiflexi dan plantar flexi Gambar 1.25 Gerakan normal dorsiflexi saat berjalan
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 10 2. Pemeriksaan
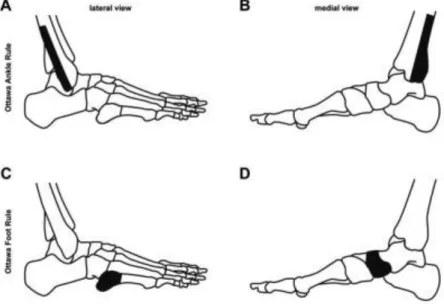
2.1Ottawa Rule Test
Pemeriksaan dengan memberikan tekanan pada area fibula, posterior tibia, cuboid & navicular. Ditujukan untuk mengetaahui adanya faktur atau patah pada tulang yang di sekita sendi ankle.
Gambar 2.1 Area Ottawa Rule test
2.2Pemeriksaan Spesifik / Tes Khusus
Pemeriksaan khusus untuk mengetahui kesobekan pada sendi ankle.
Gambar 2.2 (A) Anterior Drawer Test (ADT) khusus ligament anterior fibular ligament (ATFL) dilakukan pada posisi lutut fleksi. Sendi ankle pada posisi 10o-15o plantar fleksi dan Fisioterapis menarik tumit ke
anterior dan menahan tulang tibia. (B) Talar tilt test untuk ATFL & calcaneofibular ligament (CFL) dilakukan posisi sendi netral. Tumit posisi stabil saat mendorong sendi ke arah inversi talus dan
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 11 Gambar 2.3 Pemeriksaan khusus cedera pada sindesmosis. Pemeriksaan akan ditemui rasa nyeri pada area sindesmosis. (A) Kleiger test/External Rotation test dilakukan dengan menahan tibia dan lakukan external rotasi pada ankle. (B) Squeeze test, dengan memberikan tekanan pada tibia dan fibula di atas pertengahan calf. (C) Crossed Leg test, menyilangkan kaki pada kaki lainnya dan memberikan dorongan
ke bawah pada lutut. 2.3Antropometri
Pengukuran khusus pada sendi ankle adalah dengan melakukan antropometri Figure 8, ditujukan untuk mengetahui seberapa besar bengkak pada sendi ankle.
A B
Gambar 2.4 Pengukuran antropometri bengkak sendi ankle. (A) sisi medial, dimana pangkal meteran diletakkan pada sisi maleous lateral kemudian dikelilingkan pada navicular, plantar dan cuboid. (B) sisi lateral, dari cuboid
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 12 2.4Range Of Motion
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 14 2.5Accessory Movement test dan Manual terapi
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 18 3. Diagnosa & Protokol
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 20 3.1Sprain Ankle
Sprain ankle merupakan kesobekan ligamen sendi ankle pada sisi lateral dan medial. Mekanisme cedera persendian ankle overstretch kea rah inversi (lateral) & eversi (medial).
Gambar 3.1 Lateral sprain ankle
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 21 Lateral Sprain Ankle Protocol
ATFL & CFL tear
Grade 1 pemulihan 2- 4 minggu, Grade 2 (partial)-3 (total) pemulihan 4-8 minggu Frekuensi terapi 3-4 kali/minggu
Phase I: Fase Akut (0-3 days) Goal
Pain & swelling control
Prevent tibialis anterior & calf atrofi Protect Ligament
Manual Muscle Test 3 point Normal dorsal flexi when walking Physiotherapy Programs:
RICE
US & FUP/TENS 10 menit
Distraction grade III (pain free) 60 x, 10 sec rest, 2 sets
Dorsal glide grade III (pain free) 60 x, 10 sec rest, 2 sets
Tibiafibular dorsal glide III (pain free) (stop when sindesmosis finding) 60 x, 10 sec rest, 2 sets
Dorsal & Plantar Flexi isometric 6 sec, 10x, 2 sets
Towel exc 3 sets
Tapping/Brace (1 week) Outcome Clinical finding:
Increase ROM Dorsal flexi Decrease pain dorsal flexi
Increase step speed, step length, & single support time (bertumpu)
Phase 2: Poliferasi 1 (3day- 1week) Goals:
Normal ROM Reduce Pain Normal gait
Balance & postural stability
Prevent peroneus syndrome/compartmend syndrome with ankle brace 1 week
Physiotherapy Program: US 5 menit
PROM (pain free) 30 x, 3 sets
Calf & soleus stretch NWB (pain free) 30 sec, 3 sets (edu 3x/hari)
Calf & soleus stretch WB c/ decline (pain free) 30 sec, 3 sets (edu 3x/hari)
Alphabet exc (A,B, &C) 5 x, 2 sets (edu 3x/hari)
Distraction grade IIIII (pain free) 60 x, 10 sec rest, 2 sets
Dorsal glide grade IIIII (pain free) 60 x, 10 sec rest, 2 sets
Tibiafibular dorsal glide IIIII (pain free) 60 x, 10 sec rest, 2 sets
Ankle exc isometric 6 sec, 5 x, 2 set Ankle exc isotonic (rubber) 10x, 2 sets Bilateral calf & soles raise 10x,2 set Walking on heel & toes 2 lap Towel exc 3 sets
Ankle rhytm 15 sec, 2-3 sets
Circular wobble board (Clock & counter clock wise) bilateral & unilateral stance 10 x, 3 sets
Walking on different surface (flat, soft, & unstable) 10 x, 4 set
Level 1 run program Outcome Clinical finding:
Romberg Test SEBT
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 22 Phase 2: Poliferasi ( 2-3 week)
Goals:
Normal ROM No Pain Normal gait MMT 4 point Lower Leg Stability Physiotherapy Program:
Calf & soleus stretch NWB (pain free) 30 sec, 3 sets (edu 3x/hari)
Calf & soleus stretch WB c/ decline (pain free) 30 sec, 3 sets (edu 3x/hari)
Distraction grade IIIII (pain free) 60 x, 10 sec rest, 2 sets (stop when no pain & functional increase) Dorsal glide grade IIIII (pain free) 60 x, 10 sec
rest, 2 sets
Tibiafibular dorsal glide IIIII(pain free) 60 x, 10 sec rest, 2 sets
Ankle exc isotonic (rubber) 10x, 3sets
Bilateral calf & soles raise 10x,2 set (c/progress weight)
Walking on heel & toes 2 lap Towel exc 3 sets
Circular wobble board (Clock .counter clock wise, front & back board no touch the floor) bilateral & unilateral stance 10 x, 3 sets
Wobble board unilateral touch 3 cone15-20x, 3 set Squat with heel raise on bosu with passing 10x, 3
set
Unilateral stance on bosu 30 sec, 3 set
Hip adduction with stance on unstable surface (spons) 10x 3 set
1 leg dead lift 10x, 2 set Basic core 30 sec, 2 set Four square hopping
Side to side 10x, 2 set
Front to back 10x, 2 set Straight line hop 10x 2 set Level 2 or 3 run programs Outcome Clinical finding:
SEBT
Phase 3: maturation/functional (3-4weeks) Goals:
No pain Return to sport Physiotherapy program:
Calf & soleus raise w/ weigth 10x, 3 sets Ankle press 10x, 2-3 sets
Forward & Side walk c/rubber on ankle 10x, 2-3 set
Wobble board unilateral touch 3 cone15-20x, 3 set Squat with heel raise on bosu with passing 10x, 3
set
Unilateral stance on bosu 30 sec, 3 set
Hip adduction with stance on unstable surface (spons) 10x 3 set
Front & Side Lunge 10x 2 set Front & Drop Jump 10 x 2 set Four square hopping
Four square 5x, 2 set
Triangles 5x, 2 set
Crisscross 5x, 2 set Line zigzag 10x 2 sets Outcome Clinical Finding:
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 23 3.2Sindesmosis
Sindesmosis (high ankle sprain) adalah cedera sendi ankle sisi lateral yang megalami kesobekan ligament interesous membrane, ATFL & PTFL. Cedera ini sulit diprediksi pemulihannya karena letak impairmennya yang diantara tulang fibula dan tibia. Mekanisme cedera ini selalu tulang tibia rotasi medial dan ankle rotasi ke lateral, sehingga menyebabkan gerakan fibula ke lateral yang berdampak pada sobeknya ligament interoseus bahkan bias mematahkan tulah fibula.
Pemeriksaan khusus yang digunakan untuk kasus ini adalah kleiger test, squeeze test & crossed leg test.
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 25 Sindesmosis Protokol
Target pemulihan 55 hari/ 6 minggu Frekuensi 3-4x / minggu Phase 1 Acute 3-1 minggu
Goal:
Control pain & swelling
Protect joint Note:
Non Weight Bearing 3 day
Avoid painfull dorsiflexion & eversion Physiotherapy Programs:
RICE
US & FUP/TENS 10 menit
Distraction grade III (pain free) 60 x, 10 sec rest, 2 sets
Dorsal glide grade III (pain free) 60 x, 10 sec rest, 2 sets
Lateral glide 60 x, 10 sec rest, 2 sets
Towel exc 3 sets
Tapping/Brace (1 week)
Hip exc 10-15x, 3 sets Clinical outcome
No painfull dorsal flexi & eversi
Phase 2 sub acute (1-2 minggu) Goals:
Maintain ROM & improve flexibility
Progressing weight bearing
Strength & balance
Prevent atrofi gastroc & soleus muscle
Note:
Continue crutches for weight bearing
Physiotherapy Prorams:
Stretch gastroc, soleus & hamstring 15-20 sec, 2 sets
US & FUP/TENS 10 menit
Lateral glide ) 60 x, 10 sec rest, 2 sets
Proximal & distal tibia fibular glide 60 x, 10 sec rest, 2 sets
Seated heel raise c/ weigth 10-15x, 3 sets
Ankle rhytm/seated toe raise 15-20 sec, 3 sets
Isotonic ankle exc c/rubber 10-15x, 3 sets
Squat balance board/wobble 10-15x, 15 sec hold, 3 sets
1 leg bridge 10-15x, 15 sec hold, 3 sets
Wobble board exc (anteroposterior, clockwise & counter clockwise)
Clinical outcome
Full ROM
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 26
Phase 3 srengthening Goal:
Maximal strength
Neuromuscular control
Single limb exercise Note:
Full weight bearing still use ankle brace Physiotherapy prorams:
Advance ankle exc isotonic c/rubber 20x, 3 sets
Standing heel raise (calf & soleus muscle, double & single limb) c/weight 10-15x, 3 sets
Forward & side lunges 10-15x, 3 sets
Ankle press 10-15x, 3 sets
Side walk straight leg c/rubber 10-15x, 3 sets
Single leg wobble touch cone 15-20x, 3 sets
Single leg wobble passing/kick 15-20, 3 sets
Single leg deadlift 10-15x, 2-3 set
Hip adduction with stance on unstable surface (spons) 10x 3 set
Treadmill 10-15 minute
Clinical outcome:
SEBT
Phase 4 return to sport Goal:
Dynamic & proprioception exc
No pain when jog & run
No pain when cutting, pivoting, & specific drill
Note:
Sum total of return to sport criteria
Physiotherapy programs:
Standing heel raise (calf & soleus muscle, double & single limb) c/weight 10-15x, 3 sets
Forward & side lunges 10-15x, 3 sets
Ankle press 10-15x, 3 sets
Side walk straight leg c/rubber 10-15x, 3 sets
Single leg wobble passing/kick 15-20, 3 sets
Single leg deadlift 10-15x, 2-3 set
Four square hopping
Side to side 10x, 2 set
Front to back 10x, 2 set
Four square 5x, 2 sets
Triangle 5x, 2 sets
Crisscross 5x 2 sets
Straight line hop 10x 2 set Clinical outcome:
Hop test
3.3Chronic Ankle Instability
Kondisi cedera sprain ankle yang sudah lebih dari 2-3 bulan tidak pulih sempurna. Ditandai dengan keterbatasan gerak sendi, instabilitas ankle (ADT & Talar Tilt), nyeri saat berjalan & lari.
Pemeriksaan yang dapat dilakukan adalah ROM, Pemeriksaan spesifik, & Ankle Instability Instrument (AII) (min 5 jawaban “Ya”).
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 28 Chronic Ankle Instability Protokol
Target pemulihan 4-6 minggu Frekuensi 3-4x / minggu Phase 1: ROM & Neuromuscular control 1 minggu
Goals:
Full ROM Dorsi flexi & plantar flexi
Decrease pain
Balance
Physiotherapy programs:
Distraction grade IIIIV (pain free) 60 x, 10 sec rest, 2 sets
Dorsal glide grade IIIIV (pain free) 60 x, 10 sec rest, 2 sets
Tibiafibular dorsal glide III (pain free) (stop when sindesmosis finding) 60 x, 10 sec rest, 2 sets
Isometric Eversi (eccentric) & Inversi (Concentric) 6 sec, 10 x, 3 sets
Ankle Rhytm 15-20 sec, 2-3 sets
Towel exercise 4 sets
Double leg heel raise isometric 6 sec, 10 x, 3 sets
Double leg bridge 12x, 2 sets
Miniband series 10x 2 sets
Single leg stance on wobble lv.1-2 30 sec, 3x, 2 sets
Single leg stance on balance board perturbation 30 sec, 3x, 2 sets
Clinical Outcome:
No painfull dorsal flexi & inversi
Stork test
Phase 2: Advance Strengthening 2-3 minggu
Goals:
Increase peroneal strength
Increase flexibility
Maintain ROM
Physiotherapy Programs:
Distraction grade IIIIV (pain free) 60 x, 10 sec rest, 2 sets
Dorsal glide grade IIIIV (pain free) 60 x, 10 sec rest, 2 sets
Tibiafibular dorsal glide III (pain free) (stop when sindesmosis finding) 60 x, 10 sec rest, 2 sets
4 way Ankle Exc c/ rubber band 15x, 3 sets
Double/single leg heel raise eccentric (calf & soleus) 10x, 2 sets
Double/single leg bridge (box) 12x, 2 sets
Lunges 10x, 2 sets (see ankle dorsi flexion)
Miniband walk 4 cone 10x, 2 sets
Single leg stance on bosu 30 sec, 3x, 2 sets
Single leg stance on wobble touch 3 cone 15x, 2 sets
Double leg Box jump 10x, 2 sets
Ladder forward run 10x
Clinical outcome :
Star excursion balance test (SEBT)
Phase 3: Return to sport 4-6 minggu
Goals:
No pain running, jump, hopping
Body conditioning
Physiotherapy programs:
4 way ankle exc c/rubber
Ankle press 10-15x, 3 sets
Side walk straight leg c/rubber 10-15x, 3 sets Single leg wobble passing/kick 15-20, 3 sets Single leg deadlift 10-15x, 2-3 set
Four square hopping
Side to side 10x, 2 set
Front to back 10x, 2 set
Four square 5x, 2 sets
Triangle 5x, 2 sets
Crisscross 5x 2 sets Straight line hop 10x 2 set
Clinical outcome:
Hop test
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 29 Brosky, Tony; Nyland, john., Nitz, Art; Caborn, David N.M. 1995. The ankle ligaments: consideration of
syndesmotic injury and impilcations for rehabilitation (clinical commentary). Lexington. JOSPT Volume 21 Number 4 April.
Carl G, Mattacola; Maureen K, Dwyer. 2002. Rehabilitation of the ankle after acute sprain or chronic instability. Lexington. Journal Of Athletic Training. 2002:31(4):413-429.
Carrie L. Docherty; Bruce M. Gansnedert; Brent L. Arnold; Shepard R. Hurwitz. 2006. Development and reliability of the ankle instability instrument. Virginia. Journal of Athletic Training
2006;41(2):154-158.
Donhue. Matthew; Simon. Janet; Docherty. Carrie L. 2011. Critical review of self reported ankle instability measures. Bloomington. Journal of Foot & ankle International. DOI: 10.3113/FAI.2011.1140. Glenn N, Williams; Eric J, Allen. 2010. Rehabilitation of syndesmotic (high) ankle sprain. Lowa. DOI:
10.1177/1941738110384573.
Godges, Joe., Klingman, Robert. Tt. Physical Therapy Protocol for ankle and foot Condition. KP SoCal Ortho PT Residency.
Gribble A. Philip et al. 2014. Selection criteria for patient with chronic ankle instability in controlled research: a position statement of the international ankle consortium. USA. BJSM 2014;48:1014-1018. doi:10.1136/bjsports-2013-093175.
Green, Toni., Refshauge, Kathryn., Crosbie, Jack., Adams, Roger. 2001. A randomized controlled trial of a passive accessory joint mobilization on acute ankle inversion sprain. Australia. PTJournal-APTA
2001; 81:984-994.
Hengeveld, Elly., Banks, Kevin., Wells, Peter. 2005. Maitland’s Peripheral Manipulation 4th edition. London. Elsevier. Hal 525-575.
Kerkhoffs, Gino M. et al. 2012. Diagnosis, treatment and prevention of ankle sprain: an evidence based clinical guideline. Amsterdam. BJSM doi:10.1136/bjsports-2011-090490.
Lin, Cheng-Feng., Gross, Michael T., Weinhold, Paul. 2006. Ankle syndesmosis injuries: anatomy,
biomechanics, mechanism of injury, and clinical guidelines for diagnosis and intervention. North Carolina. JOSPT doi:10.2519/jospt.2006.2195.
Loudon, Janice K., Bell , Stephania L. 1996. The foot and ankle: an overview of arthrokinematics and selected joint technique. Kansas. Journal of athletic training Vol 31, Number 2, June 1996. McCriskin. Brendan J; Cameron. Kenneth L; Orr. Justin D; Waterman. Brian R. 2015. Management and
prevention of acute and chronic lateral ankle instability in athletic patient populations. United States. World journal of orthopaedic ISSN 2218-5836 (online). DOI: 10.5312/wjo.v6.i2.161.
SOP-Ankle Joint, ID#ARA 01, Rev 1#| 30 Nn,tt, High ankle sprain (syndesmosis sprain). South Shore Hospital.
O’Driscoll. Jeremiah; Kerin. Fearghal; Delahunt. Eamonn. 2011. Effect of 6 week dynamic neuromuscular training programme on ankle joint function: a case report. Dublin. SMARTT 2011,3:13.
Perry S, Esterson. 1979. Measurement of anle joint swelling using figure of 8. Virginia. JOSPT 0000-0000/79/0001-0051$02.00
Polzer, Hans., Kanz G. Karl., Prall C, Wolf., Haaster, Florian., Ockert, Ben., Mutscher, Wolf., Grote, Stefan. 2012. Diagnosis and treatment of acute ankle injuries: development of an evidence based algorithm. Germany. Orthopedic Review doi:10.4081/or.2012.e5.
Scott A, Lynch. 2002. Assessment of the injured ankle in the athlete. Pennsylvania. Journal of athletic training 2002;37(4):406–412.
Stiell IG, McKnight., Greenberg GH. 1994. Implementation of the Ottawa ankle rules. Canada. Ottawa Health Research Institute. JAMA 1994;271:827-832.
Terada. Masafumi; Pietrosimone. Brian G; Gribble. Philip A. 2013. Therapeutic intervention for increasing ankle dorsiflexion after ankle sprain: a systematic review. Ohio. Journal of athletic training
2013;48(5):696–709. doi: 10.4085/1062-6050-48.4.11.
Thomas W. Kaminski; Heather D. Hartsell. 2002. Factors contributing to chronic ankle instability: a strength perpective. Indianapolis. Journal of Athletic training 2002;37(4):394-405.