“WINGING OF THE SCAPULA”
AS A COMPLICATION OF OLD DISRUPTION OF THE ANTERIOR COMPONENTS OF THE SHOULDER GIRDLE (A BIOMECHANIC ANALYSIS)
-A CASE
REPORT-Hermawan Nagar Rasyid
Department of Orthopaedic Surgery, Faculty of Medicine Padjadjaran University, Dr. Hasan Sadikin Hospital, Bandung, Indonesia
ABSTRACT
“Winging of the scapula” is a condition in which the medial border moves away from the posterior chest wall. Winging of the scapula can be seen in various conditions such as palsies of the accessory or long thoracic nerve, progressive muscular dystrophy, osteochondroma of the scapula, and following chest tube insertion. We introduce disruption of the anterior component of the shoulder girdle, which can cause this condition. Anterior component of the shoulder girdle consists of sternum, clavicle and anterior part of acromion, while posterior component is a scapular blade. The anterior component will hold the scapula in it’s position. A change of shape of this part will take the scapula to droop forward and rotate. Overstretching of the axioscapular muscles can be the cause of pain in these situations. Restoration of normal anatomy reverse the pathology. Three cases presented here demonstrate the importance of the anterior component to stabilize the scapular blade back to its original position. We have recently experienced three cases of winging of the scapula and axioscapular pain following chronic dislocation of the acromioclavicular joint (Type III of Allman). All cases were treated surgically by ligament reconstruction, respectively, to restore normal anatomy. The purpose of the study is to [1] verify the pathogenesis of this type of scapular winging and [2] report the results of follow-up examinations performed after one and four years.
Keywords: Winging of the scapula, shoulder girdle, anterior component, axio-scapular muscles
INTRODUCTION
In 1867 Duchenne1 described in detail displacements of the scapula in several neurological conditions. Winging of the scapula is the one of them characterized by the prominence of the medial border of the scapula, together with rotation and forward drooping. Winging of the scapula can occur in many other conditions than neurological disorders.
impaired and unexplained dull ache around axio-scapular muscles occurred, it is possible to restore the affected site to its normal anatomy.
The purpose of the study is to verify the pathogenesis of this type of scapular winging and report the results of surgical management of complete acromioclavicular joint dislocation with long-term follow-up.
CASE REPORTS CASE 1
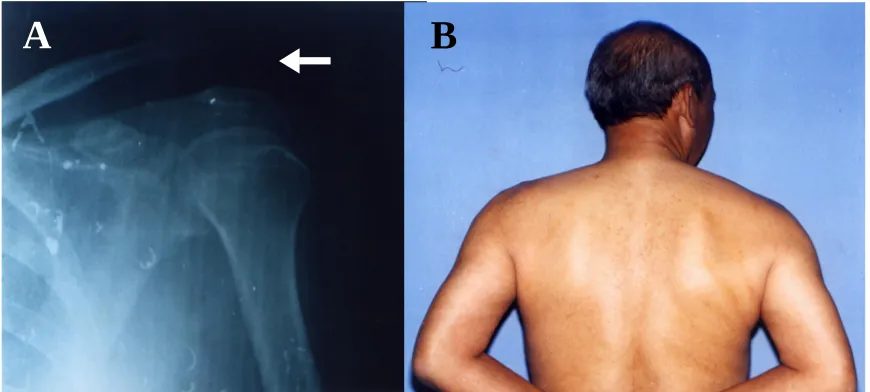
Figure 1 A, Case 1. Anteroposterior roentgenogram of left clavicle at initial examination after neglected Type III acromioclavicular joint dislocation of the left shoulder. B, Photograph made at the latest follow-up (13 months after surgery), showing disappearance of winging of left scapula.
CASE 2
A-20-year-old male student sustained a grade III right acromioclavicular joint dislocation when he fell from a motorcycle, hitting his right shoulder on February 2001. Associated injury were sustained: head injury, fracture of the left 2nd and 3rd ribs. The patient was treated
conservatively by himself in an arm sling for three weeks. Subsequently, he returned to his activity at school. He then gradually started to feel dull ache and a sense of instability in the right scapular region. At approximately 3.5 weeks following the injury, he went to Dr.Hasan Sadikin University Hospital for the unexplained dull ache around the right scapula and the persistent discomfort in the right acromioclavicular joint. On clinical examination, a significant deformity over the right acromioclavicular joint was present with a positive piano-key sign. There was no atrophy of the shoulder girdle muscles, but weakness of the shoulder girdle muscles was found. The right scapular winging was present in the resting position and became more prominent in internal rotation. There was tenderness over the right axio-scapular muscles. The range of motion of the shoulder joint was normal. Roentgenograms demonstrated distal end of the clavicle was above the superior surface of the acromion. EMG showed no evidence of long thoracic or accessory nerves palsy. Surgical procedure was performed by modified Phemister technique (Figure. 2-A). The Kirschner-wires were removed at six months postoperatively. At the latest follow-up 25 months postoperatively, the integrity of the acromioclavicular joint was maintained but the winged scapula still remained
slightly in internal rotation (Figure. 2-B). However, his preoperative pain and discomfort in the right acromioclavicular joint and the right scapular region disappeared completely.
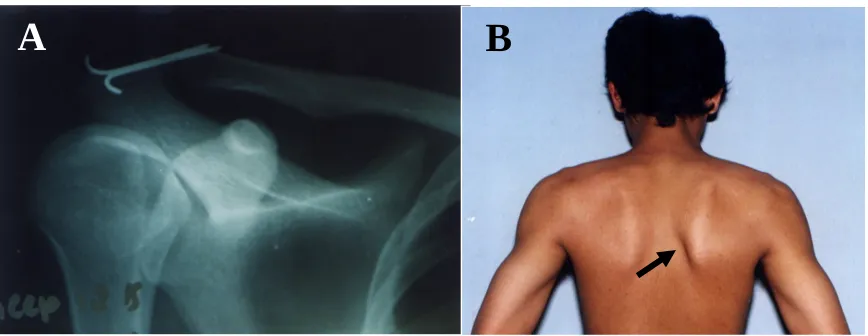
Figure 2 A, Case 2. Anteroposterior roentgenogram of right shoulder after operation of Type III acromioclavicular joint dislocation. B, Photograph made at the latest follow-up (25 months after surgery), showing leveled acromioclavicular joint on right, but winging scapula still slightly remained in internal rotation.
CASE 3
A-19-year-old male student sustained acromioclavicular joint dislocation on the right (Type III of Allman ) in a traffic accident on June1998. The patient was treated conservatively elsewhere. Subsequently, he returned to his activity at school. He then gradually started to feel dull ache and a sense of instability in the right scapular region. At approximately 5 months later, he went to Orthopaedic Clinic at Dr.Hasan Sadikin University Hospital for the prominence of the right shoulder and the persistent discomfort of the right acromioclavicular joint. On clinical examination, a significant deformity over the right acromioclavicular joint was present with a positive piano-key sign (Figure. 3-A). There was atrophy or weakness of the shoulder girdle muscles. The right scapular winging was present in the resting position and became more prominent in internal rotation (Figure. 3-B). There was tenderness over the right axio-scapular muscles. The range of motion of the shoulder joint was normal (Figure. 3-C). Roentgenograms demonstrated a Type III acromioclavicular joint dislocation. EMG showed no evidence of long thoracic or accessory nerves palsy. A combined reconstructive procedure was performed consisting of the repair of coracoclavicular ligament, the repair of the superior acromioclavicular capsular ligament, the transarticular fixation by Kirschner-wires through the acromioclavicular joint, the transference of the coracoacromial ligament and the imbrication of the deltoid and the trapezius muscles. At surgery the interior of the
identified. The Kirschner-wires were removed at three months postoperatively. At the latest follow-up 47 months postoperatively, winging of the scapula was not present both in the anatomical position or under the stress of pushing the anterior wall. The strength of the shoulder girdle muscles was normal. The range of motion of the left shoulder joint was normal. His preoperative pain and discomfort in the right acromioclavicular joint and the right scapular region disappeared completely.
Figure 3 A and B, Case 3. Photograph made at preoperation, showing anterosuperior projection of the right acromioclavicular joint.
DISCUSSION
Figure 3 C, Case 3. Photograph made at the latest follow-up (47 months after surgery), showing disappearance of winging of the right scapula.
C
Many conditions such as long thoracic nerve palsy, accessory nerve palsy, muscular dystrophy, osteochondroma of the scapula or the rib, Sprengel deformity, shoulder instability,3 chest tube insertion in the long period of time11, etc, can be the caused of winging of the scapula. Displacement of the scapula can be disabling with pain, deformity, and loss of fulcrum for the upper extremity, especially in heavy above-horizontal work.
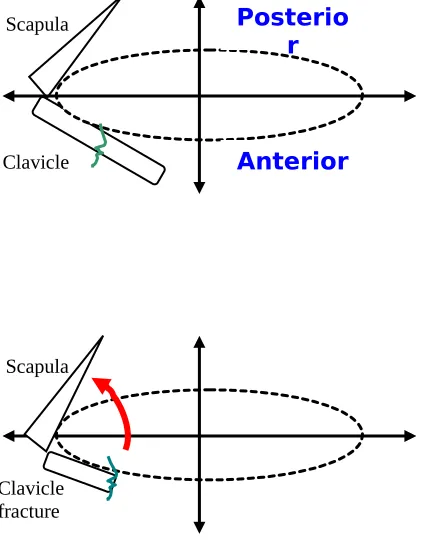
Biomechanically, the scapula is markedly mobile and suspended on the chest wall by its musculature. However, the stability of the scapula is permitted by muscles, strong ligaments and capsule to hold the relationship between the scapula and the sternum through the clavicle as a bony strut. The authors called this connection as an anterior component of the shoulder girdle. This component consists of sternoclavicle, clavicle, and anterior part of acromion. They are interdependent among themselves in stability. Stability of the scapula can be lost if the anterior component of the shoulder girdle was disrupted anywhere in its entire span, such as fracture of the midshaft clavicle or dislocation of the acromio-clavicular joint. The proposed pathogenesis is schematically drawn in Figure. 4.
Figure 4, The proposed pathomechanism of winging of the scapula.
Anterior Posterio
r
Clavicle Scapula
Scapula
In the three cases presented here, the winged scapula occurred in the similar location. The outer part of clavicle and the scapula as a unit became unstable, shifted, drooped forward and medially because of weight of the arm1,5,6,7,8,9 and traction of the pectoralis major muscle.4,10
In Case 2 and 3, together with the repeated use of the upper extremity as a toiling student for about 3.5 months, the scapula became gradually unstable. Because the winged scapula was neglected for a considerable time, the rhomboids and levator scapulae muscles on the involved side must have become stretched out.
In case 2, although the reconstruction of the acromioclavicular joint could not correct the winged scapula completely, the dull ache in the back and easy fatiguability were relieved at the time of follow-up.
Unrecognized or subtle instability of the scapula associated with clavicular and peri-clavicular injuries may not be rare in the clinical practice. If the anterior component of the shoulder girdle is disrupted in any site by trauma, the periscapular structures are to be exposed under stress, leading to the winging of the scapula in some chronically unstable cases. If the winged scapula became prominent and symptomatic in these situations, restoration of the disrupted anatomy is essential.
CONCLUSIONS
Symptomatic winging of the scapula was observed in three trauma cases of the shoulder girdle. Overstretching of the axioscapular muscles can be the cause of back pain. The pathomechanism of this complication was disruption of anterior component of the shoulder girdle, in all cases were acromio-clavicular separation. Surgery restoring normal anatomy yielded good functional results.
REFERENCES
1. Duchenne GB. Physiology of motion, translated by Kaplan EB. Paris: WB Saunders Co, 1867.
2. Allman FL Jr. Fractures and ligamentous injuries of the clavicle and its articulation. J.Bone Joint Surg (Am) 1967;49A:774-84.
3. Wilkins MR, Johnston MR. Ununited fractures of the clavicle. J.Bone Joint Surg (Am) 1983;65A:773-8. 4. Craig EV. Fractures of the clavicle. In: Rockwood CA and Matsen FA. The shoulder, vol 1. Philadelphia: WB Saunders
Co, 1990:367-412.
5. Bateman EJ. Applied physiology of the shoulder and neck. In: The shoulder and neck. Philadelphia: WB Saunders Co, 1972:67-88.
6. De Palma AF. Biomechanics of the shoulder. In: Surgery of the shoulder. 3rd ed. Philadelphia: JB Lippincott Co,
7. Fukuda H, Terada H, Yamanaka K, Hamada K. Accessory nerve palsy and stability of the sternoclavicular joint. In: The shoulder joint, Japan, 1984;8:169-72.
8. Rockwood CA Jr. Injuries to the acromioclavicular joint. In Rockwood CA and Green DP. Fracture in adults, 4th ed.
vol 2. Philadelphia: JB Lippincott Co, 1996:1341-1413.
9. Morrey BF and An KN. Biomechanics of the shoulder. In: Rockwood CA and Matsen FA. The shoulder, vol 1. Philadelphia: WB Saunders Co, 1990:208-95.