The relationship between employment grade and plasma fibrinogen
level among Japanese male employees
Masao Ishizaki
a,b,*, Pekka Martikainen
a,c, Hideaki Nakagawa
d, Michael Marmot
a,
on behalf of the YKKJ Research Group
aDepartment of Epidemiology and Public Health,International Centre for Health and Society,Uni6ersity College London Medical School,
1–19 Torrington Place,London WC1E 6BT, UK
bHealth Care Center,Kanazawa Medical Uni6ersity,1-1 Daigaku,Uchinada,Ishikawa 920-0293, Japan cDepartment of Sociology,Population Research Unit,P.O. Box18,FIN-00014,Uni6ersity of Helsinki,Helsinki, Finland
dDepartment of Public Health,Kanazawa Medical Uni6ersity,1-1 Daigaku,Uchinada,Ishikawa 920-0293, Japan
Received 24 April 1999; received in revised form 2 September 1999; accepted 15 September 1999
Abstract
Plasma fibrinogen is an important risk factor for cardiovascular disease, and is associated with socioeconomic status in Europe and the United States. We evaluated whether the relationship between socioeconomic status and plasma fibrinogen level exists in Japanese male employees, and whether this relationship is independent of other correlates of plasma fibrinogen. This cross-sec-tional study was conducted on full-time male employees aged 20 – 58 in a metal-products factory between April 1996 and March 1997. Altogether 4375 employees (92.9%) participated. Low employment grade and low educational background were associated with increased age-adjusted plasma fibrinogen level. Adjusting for body mass index, waist to hip ratio, height, smoking habit, alcohol consumption, physical activity at leisure and systolic blood pressure did not attenuate these associations much. Adjusting for white blood cell count and hemoglobin A1c reduced the associations of both employment grade and educational background with plasma fibrinogen level, nevertheless these relationships remained significant. © 2000 Elsevier Science Ireland Ltd. All rights reserved.
Keywords:Socioeconomic status; Employment grade; Educational background; Fibrinogen
www.elsevier.com/locate/atherosclerosis
1. Introduction
Socioeconomic status, such as social class, income and educational background, have been shown to be related to the development of cardiovascular disease in many industrial societies [1 – 4]. In Japan, however, relatively little information on social inequalities in cardiovascular disease is available. Nevertheless, a com-parison between Japan and the United Kingdom in the early 1980s demonstrated clear occupational differences in cerebrovascular disease mortality in Japan [5]. In 1985 and 1990 age-adjusted standardized mortality rates for heart disease among ‘transport and communi-cation’ and ‘service’ employees were higher, than
among ‘managerial, professional and technical’ em-ployees and those working in ‘crafts, production pro-cess and construction and laborers’ [6]. However, a clear socioeconomic gradient in cardiovascular disease has not been well established in Japan.
It has been demonstrated that part of the socioeco-nomic differences in cardiovascular disease are at-tributed to smoking, obesity and blood pressure [7,8]. In addition, some researchers have suggested that the pathophysiological mechanisms underlying the relation-ship between socioeconomic circumstances and the de-velopment of cardiovascular disease can also be partly explained by differences in plasma fibrinogen level [9,10]. Increasing plasma fibrinogen level plays a vital role in the formation of arterial thrombus, and has thus been recognized as one of the cardiovascular risk fac-tors [11 – 13]. Several epidemiological studies show that there is a clear relationship between socioeconomic * Corresponding author. Tel.: +44-171-5045629; fax: +
44-171-8130242.
E-mail address:[email protected] (M. Ishizaki)
status and plasma fibrinogen; the level of plasma fibrinogen is higher among lower socioeconomic groups [7,14,15]. However, it is uncertain whether socioeco-nomic status contributes to the increase of plasma fibrinogen after adjustment for other determinants of plasma fibrinogen [16,17]. Among these other determi-nants of high plasma fibrinogen level are winter season, old age, menopause, adverse early-life circumstances, genetic factors and physical conditions such as inflam-mation, obesity, diabetes and hypertension. Further-more, life-style factors such as low alcohol consumption, lack of physical exercise, poor diet and especially smoking, as well as adverse psychosocial environment can contribute to increased plasma fibrinogen level [18,19]. The purpose of this study is to investigate if a relationship between socioeconomic status and plasma fibrinogen exists in Japanese male employees, and to assess whether this possible relation-ship is independent of other determinants of fibrinogen.
2. Method
2.1. Study population
The cross-sectional study was conducted in a metal-products factory in Japan. We analyzed full-time white and blue collar male employees aged 20 – 58 registered in the factory as of 1st May in 1996, who underwent a medical checkup during the period between April 1996 and March 1997. The study excluded junior employees who had worked for less than 1 year, short-term em-ployees from recruitment agencies and a few directors, as well as 43 subjects who underwent a medical checkup at another medical facility and four subjects whose plasma fibrinogen data were not available. Alto-gether 4375 males took part in the study and the participation rate was 92.9%. We were unable to analyse females in this study because of very little variation in their employment grade.
2.2. Anthropometric measurements, blood pressure and
blood analysis
Weight, height, and waist and hip circumferences were measured with subjects dressed in the factory uniform made of thin cloth. The waist circumstance at umbilicus level and the hip circumference at the widest level were measured by experienced nurses. Height was used as a possible marker of early life influences [20]. Blood pressure was measured after the subject had rested on a chair for 5 min or longer. Non-fasting venous blood samples were collected into siliconized tubes containing 3.8% sodium citrate, and were analysed for plasma fibrinogen by the Clauss method. We also measured white blood cell count (WBC) by an
automated cell counter (SYSMEX 9421, Japan) and hemoglobin A1c (HbA1c) by high-velocity liquid chro-matography. Blood samples were analyzed in two labo-ratories; 96 and 4% of the samples, respectively. There were no significant differences in the mean values of the blood analyses between these laboratories.
2.3. Questionnaire
A self-administered questionnaire was used to collect information about life-style, including smoking habit, alcohol consumption and physical activity at leisure. Smoking habit was classified as ‘non-smokers’, ‘ex-smokers’, ‘smokers of less than 21 cigarettes a day’ and ‘smokers of 21 or more cigarettes a day’. Alcohol consumption was measured in terms of grams of ethanol consumed per week, and was based on quantity of specified drink consumed weekly. Physical activity at leisure was classified as ‘almost no exercise’, ‘light exer-cise per week’, ‘brisk and sweating exerexer-cise once or twice per week’ and ‘brisk and sweating exercise more than two times per week’.
2.4. Employment grade and educational background
Employment grade and educational background were based on data obtained from the factory records. Nine employment grades that depended on salary existed. The highest three grades in this population consisted of managers, and the third grade included those who were at supervisory positions. As the number of subjects in the highest two grades was only 27, the subjects of the highest three employment grades were put together into one grade. Other employees were classified into six hierarchical grades. The basic annual salary was 9 450 00012 350 000 yen in the combined highest grade and 4 450 000 yen in the lowest grade. Educa-tional background was determined in terms of the total years of education, and was classified as ‘more than 15 years’, ‘13 – 15 years’, ‘11 – 12 years’ and ‘less than 11 years’ of education.
2.5. Statistical analysis
winter (December – February) was not significantly dif-ferent from those in other seasons, we did not take season into account as a covariate.
3. Results
In our study population, the geometric mean of plasma fibrinogen was 2.48 g/l (95% CI; 2.472.49),
and smoking rate was 57.5%. Table 1 shows age-adjusted plasma fibrinogen levels by employment grade; the lower employment grades had higher plasma fibrinogen level (PB0.001). The difference between the highest and the lowest grade was about 0.23 units or about 10%. Differ-ences in plasma fibrinogen levels by educational back-ground were similar to those by employment grade (Table 2); participants with lower educational back-grounds had higher plasma fibrinogen levels (PB0.001).
Table 1
Age-adjusted plasma fibrinogen levels according to employment gradea
Employment grade 1 (High) 2 3 4 5 6 7 (Low) Total
690 542 4375
N 206 416 833 904 784
2.56 2.58 2.48
2.41 2.52
Mean fibrinogen (g/l) 2.35 2.55 2.55
aTrend test:PB0.001.
Table 2
Age-adjusted plasma fibrinogen levels according to educational backgrounda
Educational background I (high) II III IV (low) Total
240 2548 691 4374
N 895
Mean fibrinogen (g/l) 2.41 2.49 2.50 2.51 2.48
aEducational background: more than 15 years=I, 13–15 years=II, 11–12 years=III and less than 11 years=IV. Trend test:PB0.001.
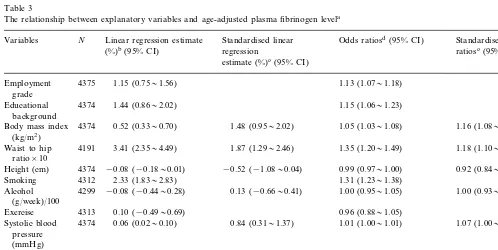
Table 3
The relationship between explanatory variables and age-adjusted plasma fibrinogen levela
Standardised linear
Linear regression estimate Standardised odds
N
Variables Odds ratiosd(95% CI)
ratiosc(95% CI)
regression (%)b(95% CI)
estimate (%)c(95% CI)
4375 1.13 (1.071.18)
Employment 1.15 (0.751.56) grade
1.44 (0.862.02)
4374 1.15 (1.061.23)
Educational background
1.48 (0.952.02) 0.52 (0.330.70)
4374
Body mass index 1.05 (1.031.08) 1.16 (1.081.23)
(kg/m2)
1.35 (1.201.49) 1.87 (1.292.46)
3.41 (2.354.49)
4191 1.18 (1.101.26)
Waist to hip ratio×10
0.92 (0.841.00) 4374
Height (cm) −0.08 (−0.180.01) −0.52 (−1.080.04) 0.99 (0.971.00)
Smoking 4312 2.33 (1.832.83) 1.31 (1.231.38)
0.13 (−0.660.41)
Alcohol 4299 −0.08 (−0.440.28) 1.00 (0.951.05) 1.00 (0.931.08) (g/week)/100
0.96 (0.881.05) Exercise 4313 0.10 (−0.490.69)
1.07 (1.001.14) 1.01 (1.001.01)
0.84 (0.311.37) 0.06 (0.020.10)
Systolic blood 4374 pressure
(mmHg)
White blood cell 4374 2.90 (2.613.20) 5.19 (4.665.72) 1.33 (1.291.37) 1.66 (1.581.73) (109/l)
4374 6.27 (5.217.35)
Hemoglobin A1c 3.31 (2.763.87) 1.75 (1.611.89) 1.35 (1.271.43)
(%)
aSmoking: no=1, ex=2, current(520/day)=3, current(\20/day)=4; exercise: no=1, light=2, brisk(B3/w)=3, brisk(\2/w)=4. bPer cent change in plasma fibrinogen level per unit change in explanatory variable.
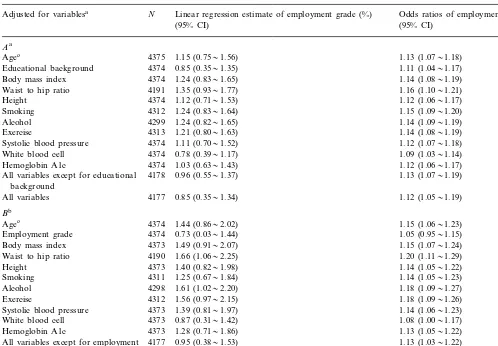
Table 4
The relationship between employment grade/educational background and plasma fibrinogen level while adjusting for age and other explanatory variables
Adjusted for variablesa N Linear regression estimate of employment grade (%) Odds ratios of employment grade
(95% CI)
Systolic blood pressure 1.11 (0.701.52) 1.12 (1.071.18)
0.78 (0.391.17)
All variables except for educational background
4177
All variables 0.85 (0.351.34) 1.12 (1.051.19)
Bb
1.44 (0.862.02)
4374 1.15 (1.061.23)
Agec
0.73 (0.031.44)
Employment grade 4374 1.05 (0.951.15)
1.49 (0.912.07)
Height 4373 1.14 (1.051.22)
1.25 (0.671.84)
Hemoglobin A1c 1.28 (0.711.86) 1.13 (1.051.22)
4177 0.95 (0.381.53) 1.13 (1.031.22)
All variables except for employment grade
All variables 4177 0.27 (−0.420.97) 1.02 (0.911.13)
aThe relationship between employment grade and plasma fibrinogen level while adjusting for age and other explanatory variables. bThe relationship between educational background and plasma fibrinogen level while adjusting for age and other explanatory variables. cThe first row of the table shows the age-adjusted effects of educational background on plasma fibrinogen level (this result is also shown in
Table 3). The following rows show the same effects while adjusting for age and the particular explanatory variable of interest.
In Table 3, we show the relationship between plasma fibrinogen level and its determinants from linear regres-sion models. The result again demonstrates that em-ployment grade and educational background were related to plasma fibrinogen level (PB0.001). Each
step down the employment grade ladder was associated with a 1.15% increase in plasma fibrinogen level, and the corresponding figure was 1.44% for educational background. Body mass index (BMI; kg/m2), waist to
hip ratio, smoking, systolic blood pressure, WBC and HbA1c were positively and significantly associated with plasma fibrinogen level (PB0.001). Height was nega-tively associated with plasma fibrinogen level, but the effect was small and bordering on significant (P=0.07). There were no significant associations between plasma fibrinogen level and alcohol consumption (P=0.65), and plasma fibrinogen level and physical activity at leisure (P=0.75). In logistic regression analyses, the relationships between all the variables and plasma
fibrinogen level were similar to those obtained in the linear regression analyses. The odds ratio was 1.13 per unit of employment grade and 1.15 per unit of educa-tional background, respectively.
Table 4A shows the relationship between employ-ment grade and plasma fibrinogen level while adjusting for age, educational background, BMI, waist to hip ratio, height, smoking, alcohol, exercise, systolic blood pressure, WBC, HbA1c, all these variables except for educational background, and all variables together. Employment grade was independently associated with plasma fibrinogen level after adjusting for each variable individually, and remained significant after adjusting for all the variables together (PB0.001). However, the regression coefficient declined on adjusting for educa-tion background, WBC and HbA1c. Similar results were shown in logistic regression analyses.
all other variables individually, as well as all variables together is shown Table 4B. Although educational back-ground was independently associated with plasma fibrinogen level after adjusting for each variable, the regression coefficients were reduced after adjusting for employment grade and WBC. Finally, the association no longer remained significant when all variables were added to the model (P=0.44). In logistic regression analyses, the odds ratio for educational background was not significant after adjusting for employment grade (P=0.37), and was borderline significant after adjusting for WBC (P=0.07).
4. Discussion
Employment grade and educational background were inversely and significantly associated with plasma fibrinogen level in our study of Japanese males. This result is in agreement with other studies which have also found that plasma fibrinogen increases with lower so-cioeconomic status, and is consistent with unpublished data from our study population showing a socioeco-nomic gradient in electrocardiogram abnormalities. We have further shown that these differences cannot be explained by BMI, waist to hip ratio, height, smoking habit, alcohol consumption, physical activity at leisure and systolic blood pressure. However, adjusting for WBC and HbA1c considerably reduced the associations of employment grade and educational background on plasma fibrinogen level.
Smoking rate has been generally demonstrated to be much higher in the lower socioeconomic statuses than in the higher socioeconomic statuses [2,21,22]. For this reason, several investigators have demonstrated that the variation of plasma fibrinogen level among socioeco-nomic groups can be explained by differences in smoking habits. In the Caerphilly and Speedwell Studies con-ducted on over 4421 males aged 45 – 59 years [16] and Scottish Heart Health Study of 8824 males and females aged 40 – 59 years [17], an inverse association was shown between social class as measured by the British Registrar General’s Social Class, and plasma fibrinogen level. This relationship, however, disappeared when taking smok-ing habit into consideration. Similar results have also been observed for young adults, aged 23 – 35 years, in the US [23]. Furthermore, a study of 639 Swedish males aged 50 [9] showed that there was no association between occupational class and plasma fibrinogen level in smok-ers. For the whole population, occupational class was not associated with plasma fibrinogen level after con-trolling for smoking habit, BMI, physical activity, plasma cholesterol and diabetes. Also Myllykangas et al. [24] reported that plasma fibrinogen level increased with fewer years of education and family income in
middle-aged Finnish males and females, but that after adjusting for smoking, the relationship disappeared among males. On the other hand, another Finnish study showed there were independent inverse associations between socioeconomic status as measured by education and income and plasma fibrinogen level in 2011 in middle-aged males in Eastern Finland, after adjusting for various confounding factors, e.g. BMI, alcohol and smoking consumption, exercise, low and high density lipoprotein cholesterol and WBC [25]. However, the study population included 42.4% farmers who were suspected of having a lower standard of education and a lower income than other employees in this country [26]. Hence, it was possible that the relationships between education, income and plasma fibrinogen level were attributed to a higher plasma fibrinogen level in farmers than in other employees. Furthermore, the study of 438 males aged 51 years in Denmark showed that social class, classified as a combination of occupation, educa-tion and the number of subordinates, was independently associated with plasma fibrinogen level after adjusting for smoking, exercise and low and high density lipo-protein cholesterol [27]. In addition, two Whitehall studies on British civil servants demonstrated that plasma fibrinogen level increased with lower employ-ment grade even after adjusting for BMI, total choles-terol and smoking [28], and after adjusting for ethnicity, BMI, smoking, alcohol, exercise, diet and symptom in the previous 14 days [14], and even after adjusting other indicators of socioeconomic statuses such as housing, educational background and father’s social class [10]. In our study, employment grade was associated with plasma fibrinogen level, even though the range of income in our study was narrower than that in the Whitehall II study, with the highest grade earning three times as much as the lowest. Over one-half of our study popula-tion (57.5%) were smokers. This proporpopula-tion corresponds well with the 56.3% smoking rate of males aged 20 – 59 years in the National Nutrition Survey in Japan in 1996 [29]. However, employment grade differences in smoking in our cohort (analysis not shown here) were relatively small and thus adjusting for smoking only made a small contribution to grade differences in plasma fibrinogen. In addition to smoking, one reason why the plasma fibrinogen level varies with socioeconomic status in the Whitehall II study was the increased level of obesity in lower employment grade [30]. However, BMI and W/H were associated negatively with employment grade in our study (analysis not shown here); i.e. higher employ-ment grades had higher BMI and waist to hip ratio than lower employment grades. Thus, adjusting for these factors tended to increase rather than decrease socioeco-nomic status differences in plasma fibrinogen level.
adjustment for WBC and HbA1c. The presence of inflammation is well known for being closely related to increased plasma fibrinogen and WBC [18,31]. In addi-tion, people with diabetes mellitus have higher plasma fibrinogen levels than those without diabetes mellitus, and HbA1c has been shown to be a good indicator of blood glucose status a few months earlier [32]. Thus, the existence of a relationship between HbA1c and plasma fibrinogen level may partly reflect that between glucose intolerance and plasma fibrinogen.
Furthermore, psychological stress has been related to release of hormones such as catecolamine and cortisol which increase blood glucose [33]. Hence, increasing HbA1c may also reflect physical condition due to in-creased psychological stress. The pressure of taking examinations [34], job dissatisfaction [35] and job strain [36] have in fact been found to be associated with elevated HbA1c. In other investigations, job stress such as ‘little control, little variety and under use of skills’ [28], ‘low control and high work pace’ [36] and ‘high effort and low reward’ [37] was demonstrated to be associated with increased plasma fibrinogen level. Con-sequently, it seems possible that the relationship between employment grade and plasma fibrinogen that we found may be partly attributed to psychosocial stress.
In this study, both employment grade and educational background were associated with plasma fibrinogen level when several behavioural and biological determinants of plasma fibrinogen level were adjusted. However, the relationship between educational background and plasma fibrinogen level was considerably attenuated when employment grade was adjusted. This may indicate that a large part of the effects of educational background on plasma fibrinogen level were mediated by employ-ment grade. In contrast, the association between em-ployment grade and plasma fibrinogen level was largely independent of educational background, indicating that employment grade more broadly reflects the effects of socioeconomic status on plasma fibrinogen level than educational background.
In the interpretation of our findings, attention needs to be paid to the following aspects of our study. First, the data for this study were collected at cross-section. Therefore, causal interpretations and evaluation of un-derlying mechanisms of the relationship between socioe-conomic status and plasma fibrinogen level are difficult. Secondly, part of the independent association of socioe-conomic status on plasma fibrinogen level may be due to our inability to measure accurately all our mediators, and a lack of detailed information on some explanatory factors know to be related to plasma fibrinogen, such as early life circumstances and psychosocial stress.
In conclusion, we found there was an inverse associa-tion between employment grade and plasma fibrinogen level after adjusting for age, educational background, BMI, waist to hip ratio, height, smoking, alcohol,
exercise, systolic blood pressure, WBC and HbA1c. Although Japan has very low coronary heart disease rates as compared with Europe and the United States and the socioeconomic gradient in cardiovascular dis-ease has not been definitively established, these results suggest that plasma fibrinogen may contribute to biolog-ical explanations of socioeconomic differences in cardio-vascular disease. Further investigation into other determinants of socioeconomic differences in plasma fibrinogen level, such as psychosocial stress, should be conducted.
Acknowledgements
The YKKJ Research Group is composed of Masao Ishizaki, Pekka Martikainen, Hideaki Nakagawa, Michael Marmot, Yuichi Yamada (Kanazawa Medical University), Yuko Morikawa (Kanazawa Medical Uni-versity), Fusako Enokido (Kanazawa Medical Univer-sity), Yuka Noborisaka (Kanazawa Medical University), Katsuyuki Miura (Kanazawa Medical Uni-versity), Teruhiko Kido (Kanazawa University) and Yuchi Naruse (Toyama Medical and Pharmaceutical University). We would like to thank Eric Bruner for his useful advice. We also thank Toshio Saito, Akira Doinaga, Ryumon Honda, Ian O’Sullivan and Katy Jones for help in the preparation of this manuscript. This study was supported by a grant from Kanazawa Medical University(C96-11). MM is supported by a MRC Re-search Professorship. PM is supported by the National Institute on Aging (AG 13196), and the John D. and Catherine T. MacArthur Foundation Research Net-works on Successful Midlife Development and Socio-economic Status and Health.
References
[1] Valkonen T. Adult mortality and level of education: a comparison of six countries. In: Fox J, editor. Health Inequalities in European Countries. Aldershot: Gower Publishing, 1989:142 – 6.
[2] Marmot MG, Smith GD, Stansfeld S, Patel C, North F, Head J, White I, Brunner E, Feeney A. Health inequalities among British civil servants: the Whitehall II study. Lancet 1991;337:1387 – 93. [3] Davey-Smith G, Neaton JD, Wentworth D, Stamler R, Stamler J. Mortality differences between black and white men in the USA: contribution of income and other risk factors among men screened for the MRFIT. Lancet 1998;351:934 – 9.
[4] Acheson D. Independent inquiry into inequalities in health. London: The Stationery Office, 1998.
[5] Kagamimori S, Matsubara I, Sokejima S, Sekine M, Matsukura T, Nakagawa H, Naruse Y. The comparative study on occupa-tional mortality, 1980 between Japan and Great Britain. Ind Health 1998;36:252 – 7.
[7] Colhoun H, Prescott-Clarke P. Health survey for England 1994. London: HMSO, 1996.
[8] Colhoun HM, Hemingway H, Poulter NR. Socio-economic status and blood pressure: an overview analysis. J Hum Hypertens 1998;12:91 – 110.
[9] Rosengren A, Wilhelmsen L, Welin L, Tsipogianni A, Teger-Nilsson AC, Wedel H. Social influences and cardiovascular risk factors as determinants of plasma fibrinogen concentration in a general population sample of middle aged men. Br Med J 1990;300:634 – 8.
[10] Brunner E, Davey-Smith G, Marmot M, Canner R, Beksinska M, O’Brien J. Childhood social circumstances and psychosocial and behavioural factors as determinants of plasma fibrinogen. Lancet 1996;347:1008 – 13.
[11] Lee AJ, Lowe GD, Woodward M, Tunstall-Pedoe H. Fibrinogen in relation to personal history of prevalent hypertension, diabetes, stroke, intermittent claudication, coronary heart disease, and family history: the Scottish Heart Health Study. Br Heart J 1993;69:338 – 42.
[12] Meade TW, Ruddock V, Stirling Y, Chakrabarti R, Miller GJ. Fibrinolytic activity, clotting factors, and long-term incidence of ischaemic heart disease in the Northwick Park Heart Study. Lancet 1993;342:1076 – 9.
[13] Woodward M, Lowe GD, Rumley A, Tunstall-Pedoe H. Fibrino-gen as a risk factor for coronary heart disease and mortality in middle-aged men and women. The Scottish Heart Health Study. Eur Heart J 1998;19:55 – 62.
[14] Brunner EJ, Marmot MG, White IR, O’Brien JR, Etherington MD, Slavin BM, Kearney EM, Davey Smith D. Gender and employment grade differences in blood cholesterol, apolipo-proteins and haemostatic factors in the Whitehall II study. Atherosclerosis 1993;102:195 – 207.
[15] Woodward M, Lowe GD, Rumley A, Tunstall-Pedoe H, Philip-pou H, Lane DA, Morrison CE. Epidemiology of coagulation factors, inhibitors and activation markers: the Third Glasgow MONICA Survey. II. Relationships to cardiovascular risk factors and prevalent cardiovascular disease. Br J Haematol 1997;97:785 – 97.
[16] Baker IA, Sweetnam PM, Yarnell JW, Bainton D, Elwood PC. Haemostatic and other risk factors for ischaemic heart disease and social class: evidence from the Caerphilly and Speedwell studies. Int J Epidemiol 1988;17:759 – 65.
[17] Lee AJ, Smith WC, Lowe GD, Tunstall-Pedoe H. Plasma fibrino-gen and coronary risk factors: the Scottish Heart Health Study. J Clin Epidemiol 1990;43:913 – 9.
[18] Folsom AR. Epidemiology of fibrinogen. Eur Heart J (Suppl A) 1995;16:21 – 3.
[19] Lip GY. Fibrinogen and cardiovascular disorders. Q J Med 1995;88:155 – 65.
[20] Marmot MG, Bosma H, Hemingway H, Brunner E, Stansfeld S. Contribution of job control and other risk factors to social variations in coronary heart disease incidence. Lancet 1997;350:235 – 9.
[21] Prescott-Clarke P, Primatesta P. Health survey for England ‘96. London: The Stationery Office, 1998.
[22] Lantz PM, House JS, Lepkowski JM, Williams DR, Mero RP, Chen J. Socioeconomic factors, health behaviors, and mortality: results from a nationally representative prospective study of US adults. J Am Med Assoc 1998;279:1703 – 8.
[23] Folsom AR, Qamhieh HT, Flack JM, Hilner JE, Liu K, Howard BV, Tracy RP. Plasma fibrinogen: levels and correlates in young adults. The Coronary Artery Risk Development in Young Adults (CARDIA) Study. Am J Epidemiol 1993;138:1023 – 36.
[24] Myllykangas M, Pekkanen J, Rasi V, Haukkala A, Vahtera E, Salomaa V. Haemostatic and other cardiovascular risk factors, and socioeconomic status among middle-aged Finnish men and women. Int J Epidemiol 1995;24:1110 – 6.
[25] Wilson TW, Kaplan GA, Kauhanen J, Cohen RD, Wu M, Salonen R, Salonen JT. Association between plasma fibrinogen concentration and five socioeconomic indices in the Kuopio Ischemic Heart Disease Risk Factor Study. Am J Epidemiol 1993;137:292 – 300.
[26] Luoto R, Pekkanen J, Uutela A, Tuomilehto J. Cardiovascular risks and socioeconomic status: differences between men and women in Finland. J Epidemiol Commu Health 1994;48:348 – 54.
[27] Moller L, Kristensen TS. Plasma fibrinogen and ischemic heart disease risk factors. Arterioscler Thromb 1991;11:344 – 50. [28] Markowe HL, Marmot MG, Shipley MJ, Bulpitt CJ, Meade
TW, Stirling Y, Vickers MV, Semmence A. Fibrinogen: a possi-ble link between social class and coronary heart disease. Br Med J 1985;291:1312 – 4.
[29] Health Service Bureau, Ministry of Health and Welfare. KOKUMIN-EIYO-NO-GENJO (in Japanese). Tokyo, Daiichi Shuppan, 1998.
[30] Brunner EJ, Marmot MG, Nanchahal K, Shipley MJ, Stansfeld SA, Juneja M, Alberti KG. Social inequality in coronary risk: central obesity and the metabolic syndrome. Evidence from the Whitehall II study. Diabetologia 1997;40:1341 – 9.
[31] Folsom AR, Wu KK, Davis CE, Conlan MG, Sorlie PD, Szklo M. Population correlates of plasma fibrinogen and factor VII, putative cardiovascular risk factors. Atherosclerosis 1991;91:191 – 205.
[32] American Diabetes Association. Implications of the diabetes control and complications trial. Diabetes 1993;42:1555 – 1558. [33] Surwit RS, Schneider MS. Role of stress in the etiology and
treatment of diabetes mellitus. Psychosom Med 1993;55:380 – 93. [34] Netterstrom B, Danborg L, Olesen H. Glycated hemoglobin as
a measure of physiological stress. Behav Med 1988;14:13 – 6. [35] Kawakami N, Araki S, Hayashi T, Masumoto T. Relationship
between perceived job-stress and glycosylated hemoglobin in white-collar workers. Ind Health 1989;27:149 – 54.
[36] Netterstrom B, Kristensen TS, Damsgaard MT, Olsen O, Sjol A. Job strain and cardiovascular risk factors: a cross sectional study of employed Danish men and women. Br J Ind Med 1991;48:684 – 9.
[37] Siegrist J, Peter R, Cremer P, Seidel D. Chronic work stress is associated with atherogenic lipids and elevated fibrinogen in middle-aged men. J Intern Med 1997;242:149 – 56.