Reduced mildly oxidized LDL in young female athletes
Tommi Vasankari
a,b,*, Marjo Lehtonen-Veromaa
c, Timo Mo¨tto¨nen
c,
Markku Ahotupa
d, Kerttu Irjala
e, Olli Heinonen
a, Aila Leino
e, Jorma Viikari
caSports and Exercise Medicine Unit,Paa6o Nurmi Centre,Kiinamyllynkatu 10,20520 Turku, Finland bSports Institute of Finland,Vieruma¨ki, Finland
cDepartment of Medicine,Turku Uni6ersity Central Hospital,Turku, Finland dMCA Research Laboratory,Department of Physiology,Uni6ersity of Turku,Turku, Finland
eDepartment of Clinical Chemistry,Turku Uni6ersity Central Hospital,Turku, Finland
Received 8 April 1999; received in revised form 8 September 1999; accepted 22 September 1999
Abstract
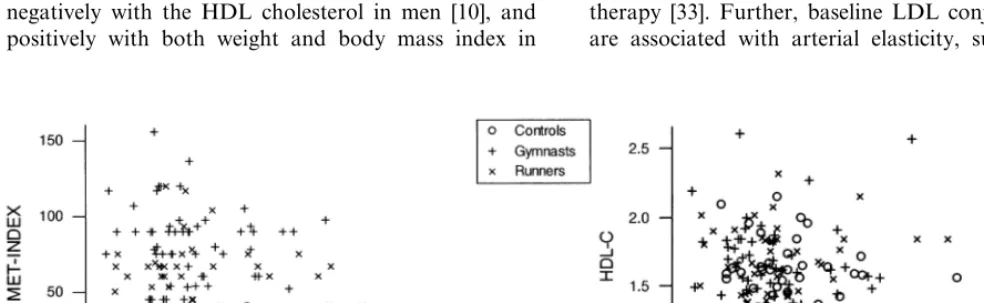
We investigated the effect of physical activity and sports participation on LDL oxidation in vivo and on lipid risk factors in 183 teenage girls (9 – 15 years): 64 gymnasts, 61 runners, and 58 controls. Oxidized LDL was measured as baseline levels of conjugated dienes in LDL lipids (ox-LDL). The gymnasts had a 15% lower ratio of LDL conjugated dienes to LDL cholesterol (ox-LDL:LDL ratio,P=0.0052) compared to controls, and the difference persisted when the body mass index was included as a covariate (ANCOVA,P=0.013). Also, the gymnasts had a 12% higher ratio of HDL cholesterol to total cholesterol than the controls (ANCOVA, P=0.046). There were no differences in the other common lipid risk factors between the groups. The ox-LDL:LDL ratio correlated negatively with HDL cholesterol (r= −0.23, P=0.0021) and with physical activity METs (multiples of resting metabolic rate) (r= −0.21, P=0.0040). Our study strengthens the evidence that the atherogenic risk is influenced favourably by physical exercise and sporting activities as early as in adolescents. This risk reduction is associated with lower mildly oxidized LDL in adolescent girls. © 2000 Elsevier Science Ireland Ltd. All rights reserved.
Keywords:Antioxidant potential; Atherosclerosis; LDL conjugated dienes; Physical activity
www.elsevier.com/locate/atherosclerosis
1. Introduction
Atherogenesis is a continuous process that starts very early in life. It is well established that the clinical manifestations of coronary heart disease (CHD) can appear in early childhood and that many of the risk factors for CHD are largely determined by behavioral patterns established in childhood [1 – 3]. Effective pri-mary prevention of atherosclerosis should, conse-quently, be directed toward young people. Physical activity is one means of preventing CHD [4], and CHD is uncommon among former endurance athletes [5]. A similar beneficial association between physical activity and CHD risk status prevails among adolescents [6,7]. The cardiovascular benefits of exercise are a conse-quence of decreased plasma triglyceride levels,
in-creased high density lipoprotein cholesterol (HDL-C) levels and increased apolipoprotein A – I concentrations [8]. We recently reported that several years of intensive physical exercise training is associated with a reduced fraction of mildly oxidized serum LDL-C in adults [9]. Further, an exercise program of 10-month’s duration reduces mildly oxidized LDL-C levels by 23 and 26% in sedentary men and women, respectively [10], while acute but prolonged physical exercise does not affect these levels [11,12]. There are no studies available con-cerning LDL oxidation in adolescents, and the possible effect of physical activity on LDL oxidation even at this early age.
In this study we investigated the effect of physical activity and sports on LDL oxidation and lipid risk factors in 183 adolescent girls (athletes and controls, 9 – 15 years). As indicators of LDL oxidation we deter-mined the ratio of LDL baseline conjugated dienes to LDL-C (mildly oxidized LDL) and the antioxidant potential of the LDL-C fraction [13]. Elevated levels of * Corresponding author. Tel.: +358-40-5059157; fax: +
358-2-2502610.
E-mail address:[email protected] (T. Vasankari)
oxidized LDL reflect a high risk of atherosclerosis, while a high antioxidant potential of LDL reflects a high total antioxidant capacity of LDL-C, which may reduce the risk of atherosclerosis [13].
2. Material and methods
2.1. Subjects
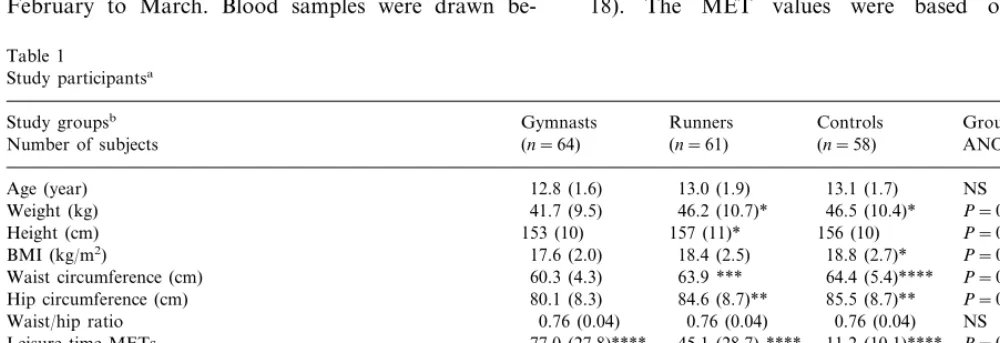
The study group comprised 183 healthy, Caucasian girls aged 9 – 15 years (64 gymnasts of local competitive level, 61 runners of local competitive level, and 58 nonathletic controls). The participants were recruited from the local sport clubs, and from the schools of the city of Turku during the period from October 1996 to January 1997. None of the participants had any chronic disease and none used drug therapy (one girl used oral contraceptives). The study protocol was approved by the joint ethics committee of the Turku University and Turku University Central Hospital. The study was car-ried out in accordance with the Declaration of Helsinki. The subjects and, where applicable, their parents volun-teered their written informed consent after the purpose, possible risks, and stress associated with the study had been explained. The subject characteristics are summa-rized in Table 1.
2.2. Study design
All girls were investigated during a 6-week period in February to March. Blood samples were drawn
be-tween 07:30 – 8:00 h after an overnight (12 h) fast. Blood sampling in the groups of girls who menstruated took place in the early follicular phase of menstrual cycle (days 5 – 8). After separation of blood cells by centrifugation, one serum tube was frozen and stored at −70°C until analyzed (lipid oxidation markers) and one tube was processed by standard lipid analysis with-out freezing. Each participant’s body weight and height were measured and the body mass index (BMI, kg/m2) was calculated. The waist circumference was measured at the level of the umbilicus and the hip circumference at the level of the widest part of the hips and buttocks. All anthropometric measurements were made in the morning by the same observer.
2.3. Questionnaires
All questionnaires were answered by the individual participant together with one of her parents or, in the case of older participant, alone. The subjects completed a detailed questionnaire of physical activity. The com-petitive athletic history and the leisure time physical activity (LTPA) during the past 6 months (weekly frequency, mean duration and mean intensity of physi-cal activity bouts) were reported retrospectively. On the basis of this information a LTPA was calculated as MET-hours per week (METindex). MET values are multiples of resting metabolic rate with an energy cost of about 1 kcal/kg per h and were calculated here as the product of intensity×duration×frequency (e.g. 4 (in-tensity)×1.5 h (duration)×3 (frequency per week)= 18). The MET values were based on a recent
Table 1
Study participantsa
Gymnasts Runners Controls Group difference Study groupsb
(n=64) (n=61)
Number of subjects (n=58) ANOVA
13.0 (1.9)
Hip circumference (cm) 80.1 (8.3) 84.6 (8.7)** 85.5 (8.7)** P=0.0008 0.76 (0.04) NS
Waist/hip ratio 0.76 (0.04) 0.76 (0.04)
Leisure time METs 77.0 (27.8)**** 45.1 (28.7) **** 11.2 (10.1)**** P=0.0001
Current smokers 1/64 0/61 1/58 NS Pubic hair development (Tanner’s stages I/II/III/IV/V)
aMean (SD) or number in groups. BMI=body mass index, MET=ratio of work metabolic rate to resting metabolic rate. Differences between
groups were tested by ANOVA.
bIndicates statistically significant difference between gymnasts and runners/controls.
* 0.01BPB0.05. ** 0.001BPB0.01. *** 0.0001BPB0.001.
comprehensive study (e.g. 4 for exercise intensity corre-sponding to walking, six jogging, 10 running and 13 fast running) [14].
We also estimated mean daily energy and fat intakes from 4-day food records by a dietitian using the Mi-cronutrica software (Social Insurance Institution, Turku, Finland) [15]. Smoking habits and alcohol con-sumption were also assessed by questionnaire. The stage of pubertal development was evaluated by self-as-sessment of breast and pubic hair stage in girls accord-ing the method of Tanner [16,17]. The participants were given pictures of girls at different stages of pubertal development together with brief descriptions, and they selected the picture that most accurately reflected their own appearance. The Tanner stage was also verified and recorded by the researcher (M. L – V.). The men-strual status was determined for each subject by inter-view. The subjects reported their date of menarche, menstrual cycle history since menarche and menstrual status for the past year.
2.4. Analytical methods
Serum total and HDL cholesterol, triglycerides, and apolipoproteins A – I and B were determined from fresh samples in Turku University Central Hospital. Total cholesterol, HDL cholesterol and triglycerides were measured by enzymatic methods with the use of Boehringer reagents (a Hitachi 717 chemistry analyzer). LDL cholesterol was calculated using the equation of Friedewald et al. [18]. Apolipoproteins A – I and B were determined by immunonephelometric assays (Behringwerke).
Baseline LDL conjugated dienes were measured as described earlier [13], and serum low density lipo-proteins were isolated by precipitation [19]. Lipids were extracted from the LDL samples (100 ml) by
chloro-form – methanol (2:1), dried under nitrogen, then redis-solved in cyclohexane and analyzed spectrophoto-metrically at 234 nm. Oxidation during the sample preparation is prevented by EDTA [13]. Additionally, baseline conjugated dienes measured in heparin precipi-tated LDL are not different from those measured in LDL isolated by the conventional ultracentrifugation method [20]. The ratio of LDL baseline conjugated dienes to LDL cholesterol (the oxLDL:LDL ratio) was used to express mildly oxidized LDL in vivo. For LDL baseline conjugated dienes, the CV of the between-as-say precision was 4.8% (n=17, level: 64.693.2mmol/l)
over a 3-month period.
The antioxidant potential of the LDL-C samples was assessed in vitro by the potency of the samples to resist 2,2%-azobis(2-amidinopropane)HCl-induced peroxida-tion (total peroxyl radical trapping antioxidant poten-tial) [13]. The peroxyl radical trapping capacity was defined by the half-peak time point. Trolox served as a standard radical scavenger.
2.5. Statistical analyses
Results are expressed as mean9standard deviation unless stated otherwise. Individual values of skewed variables were ln-transformed (serum triglyceride, HDL-C, oxidized LDL), and the normality of the transformal distribution was confirmed before statisti-cal testing. Comparison between the study groups was performed by ANOVA for continuous variables, by the
x2-test for categorical variables and by the Jonckheere –
Terpstra Test for pubertal development. Because of differences of BMI between the groups, BMI was used as covariate (ANCOVA). Tukey’s test was used for post hoc multiple comparisons. The correlations be-tween the exercise groups were tested using Spearman’s correlation coefficient.P-valuesB0.05 were considered as significant. For all statistics the appropriate proce-dures of the SAS software were run.
3. Results
The study groups did not differ with respect to age, pubertal development or smoking habits, but, as ex-pected, body weight, height, BMI, waist and hip cir-cumference were smaller in the gymnasts compared to the runners and nonathletic controls (Table 1). The MET-index of LTPA was highest in the gymnasts and lowest in the controls. The food records showed a systematic difference between the groups: the runners consumed more energy and all types of fat per body weight compared to controls (Table 2). In addition, the gymnasts used more energy per body weight compared to the controls, but there were no differences in fat consumption.
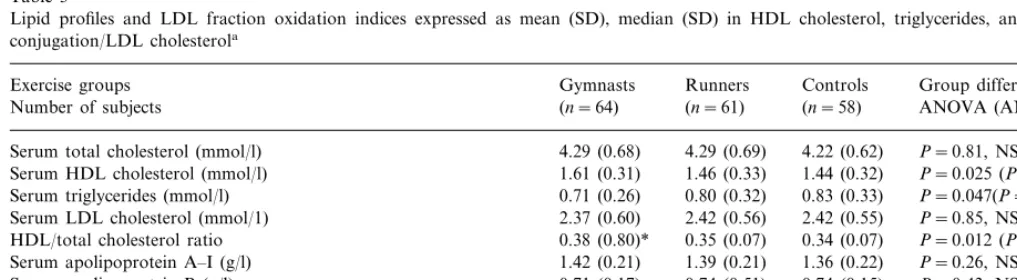
In ANOVA, the concentrations of serum total cholesterol, LDL-C, apolipoprotein A – I and B, ratio of apolipoprotein A – I to B, and LDL antioxidant capac-ity did not differ between the groups, but the serum triglycerides, HDL-C, ox-LDL:LDL ratio and the ratio of HDL-C to total cholesterol did (Table 3). The nonathletic controls had an 18% higher concentration of serum triglycerides (P=0.046), an 11% lower HDL-C (P=0.022) and an 11% lower ratio of HDL-C to total cholesterol (P=0.012) than the gymnasts. The gymnasts and runners had 15 and 11% lower ox-LDL:LDL ratio (P=0.0052 and P=0.058, respec-tively) compared to the controls. When BMI was taken as a covariate, only the ox-LDL:LDL ratio and the ratio of HDL-C to total cholesterol remained signifi-cantly different between the gymnasts and controls (P=0.013 and P=0.046).
Table 2
The estimated mean (SD) daily dietary energy and fat intakes per body weight and percents of daily energya
Gymnasts
Study groups Runnersb Controls Group difference
(n=61) (n=58)
aDifferences between groups were tested by ANOVA. SAFA=saturated fat, MUFA=monounsaturated fat, PUFA=polyunsaturated fat. bIndicates significant difference between controls and runners/gymnasts.
* 0.01BPB0.05. ** 0.001BPB0.01. ***PB0.001.
Table 3
Lipid profiles and LDL fraction oxidation indices expressed as mean (SD), median (SD) in HDL cholesterol, triglycerides, and LDL diene conjugation/LDL cholesterola
Runners
Exercise groups Gymnasts Controls Group difference
(n=61) (n=58)
(n=64) ANOVA (ANCOVA)
Number of subjects
Serum total cholesterol (mmol/l) 4.29 (0.68) 4.29 (0.69) 4.22 (0.62) P=0.81, NS 1.46 (0.33) 1.44 (0.32)
1.61 (0.31) P=0.025 (P=0.095, NS) Serum HDL cholesterol (mmol/l)
0.71 (0.26)
Serum triglycerides (mmol/l) 0.80 (0.32) 0.83 (0.33) P=0.047(P=0.10, NS) 2.37 (0.60)
Serum LDL cholesterol (mmol/1) 2.42 (0.56) 2.42 (0.55) P=0.85, NS 0.35 (0.07) 0.34 (0.07)
0.38 (0.80)* P=0.012 (P=0.046) HDL/total cholesterol ratio
1.42 (0.21)
Serum apolipoprotein A–I (g/l) 1.39 (0.21) 1.36 (0.22) P=0.26, NS 0.74 (0.51) 0.74 (0.15)
0.71 (0.17) P=0.43, NS
Serum apolipoprotein B (g/l)
1.95 (0.50) 1.94 (0.56)
Apolipoprotein A–I/B ratio 2.13 P=0.11, NS
10.2 (3.2) 11.5 (3.5)
9.8 (2.7)* P=0.0058 (P=0.013)
LDL conjugated dienes/LDL cholesterol (mmol/mmol LDL)
21.2 (4.7)
LDL antioxidant capacity/LDL cholesterol (mmol/mmol LDL) 21.4 (4.3) 22.3 (4.8) P=0.40, NS
aDifferences between groups were tested by ANOVA, and in case of signifiqcant difference between the groups in ANOVA, BMI was taken
as covariate (ANCOVA).
* Indicates statistically significant difference between controls and gymnasts.PB0.05. NS=statistically non-significant.
(r=0.18, P=0.014). There was also an association between the ox-LDL:LDL ratio and a stage of breast development (Anova,P=0.0042): the girls in Tanner’s stages II and IV had 26 and 22% higher ox-LDL:LDL ratio compared to the girls in Tanner’s stage I (Tukey, P=0.0029 andP=0.013, respectively). Also, the trend test between the ox-LDL:LDL ratio and stage of breast development was significant (Jonckheere – Terpstra,P= 0.028). Similar association was not seen between the ox-LDL:LDL ratio and pubic hair stage (Jonckheere – Terpstra,P=0.067).
4. Discussion
We investigated the effect of physical activity and sports participation on oxidized LDL and lipid risk factors in 183 healthy adolescent girls. This is apparently
Of the common lipid risk factors, serum triglycerides and HDL-C differed between the gymnasts and the nonathletic controls, but when BMI was used as a covariate, the difference disappeared. The ratio of HDL-C to total cholesterol was lower in the controls compared to the gymnasts, and the difference persisted when BMI was used as a covariate. The relatively low association between physical activity and the common lipid risk factors in teenage girls is supported by a recent Finnish cohort study according to which the only lipid response to physical activity in young females concerned serum triglycerides (P=0.029); the association was much stronger in males of similar age [21]. In the present study, the athletes with the highest exercise activity (gymnasts) had the best overall lipid profile compared to the other groups.
The observation that mildly oxidized LDL is reduced in young gymnasts is in line with our earlier study, where we found that several years of intensive physical exercise training was associated with reduced mildly oxidized LDL in veteran athletes [9]. A program of 3 – 5 h exercise per week for 10 months is also sufficient to reduce mildly oxidized LDL by 14 and 18% in men and women who have been sedentary [10]. The denser LDL cholesterol subfractions are more susceptible to oxidative modification [22] and endurance runners have lower concentrations of the densest LDL cholesterol subfraction than inactive controls [23]. This might be an explanation for the lower ox-LDL:LDL ratio in the physically active girls compared to the controls in this study. On the other hand, LDL oxidation is not affected by acute physical exercise, at least not in sedentary adults or healthy endurance athletes [11,12]. The mildly oxidized LDL was associated with the MET-index, HDL-C and body weight in adolescent girls. This is in line with the earlier results reported in sedentary adults: the mildly oxidized LDL correlated negatively with the HDL cholesterol in men [10], and positively with both weight and body mass index in
women and men [24,25]. The present results are also i n accord with an another study, where a weight reduction of 13 kg was associated with a 40% decrease in LDL baseline conjugated dienes in 78 obese premenopausal women [24]. This indicates that the LDL oxidation in vivo is also related to some conventional non-lipid risk factors of atherosclerosis.
Experimental evidence strongly supports the hypothesis that oxidation of LDL-C is atherogenic [26]. It has also been found that mildly oxidized LDL-C may circulate in the plasma sufficiently long to enter, accumulate and be degraded in the arterial intima [27]. Unlike highly oxidized LDL, such minimally modified LDL-C is taken up by LDL receptor rather than by scavenger receptor [28]. As a further indication of the existence of circulating oxidized LDL, it was found that vascular endothelial cells have a specific receptor for oxidized LDL [29,30].
Measurement of diene conjugation has become the most popular method to monitor LDL oxidation in vitro, and the oxidation induced increase of diene conjugation in LDL lipids is well documented [31,32]. Our method for the direct measurement of mildly oxidized LDL measures the baseline level of conjugated dienes in LDL. Chemical HPLC and NMR studies have shown that LDL conjugated dienes result from conjugated dienes in fatty acids of cholesteryl esters and triglycerides of the LDL (unpublished observation, Vasankari et al., 1998). Recently, we demonstrated an association between mildly oxidized LDL and severity of coronary artery disease: the oxLDL:LDL ratio was 41% higher in patients with multi-vessel disease compared to the subjects with normal coronary arteries (unpublished observation, Vasankari et al., 1998). Another group recently reported a reduction by 21% in baseline LDL conjugated dienes in coronary artery disease patients undergoing atherosclerosis-reversal therapy [33]. Further, baseline LDL conjugated dienes are associated with arterial elasticity, suggesting that
oxidative modification of LDL may play a role in the arterial wall elastic properties [34]. In that study, the elastic properties of large arteries in the ascending and descending parts of thoracic aorta were investigated by using magnetic resonance imaging. The compliance of ascending aorta correlated with baseline LDL conju-gated dienes (r= −0.44, P=0.030) but not with the traditional lipid risk factors in 25 healthy men under 40 years of age [34]. We have also demonstrated a strong correlation (r=0.57,P=0.001) between the concentra-tion of LDL-conjugated dienes and the autoantibody titer against oxidized LDL [20].
The results of the present study strengthen the evi-dence that, in adolescents, atherogenic risk is already influenced favourably by physical exercise and sporting activity. This risk reduction is associated with lower mildly oxidized LDL in adolescent girls.
Acknowledgements
This study was funded by the Juho Vainio Foun-dation, the Turku University FounFoun-dation, and the gov-ernment support of Turku University Hospital, Fin-land.
References
[1] Joseph A, Ackerman D, Talley JD, Johnstone J, Kupersmith J. Manifestation of coronary atherosclerosis in young trauma vic-tims — an autopsy study. J Am Coll Cardiol 1993;22:459 – 67. [2] Research Group PDAY. Natural history of aortic and
coro-nary atherosclerotic lesions in youth. Findings from the PDAY study. Arterioscler Thromb 1993;13:1291 – 8.
[3] WHO. Prevention in childhood and youth of adult cardiovas-cular diseases: time for action. Report of a World Health Or-ganization Expert Committee. Geneva: Technical Report Series 792; 1990.
[4] Powell KE, Thompson PD, Caspersen CJ, Kendrick JS. Physi-cal activity and the incidence of coronary heart disease. Ann Rev Public Health 1987;8:253 – 87.
[5] Kujala UM, Kaprio J, Taimela S, Sarna S. Prevalence of dia-betes, hypertension, and ischemic heart disease in former elite athletes. Metabolism 1994;43:1255 – 60.
[6] Raitakari OT, Porkka KVK, Taimela S, Telama R, Rasanen L, Viikari JSA. Effects of persistent physical activity and inac-tivity on coronary risk factors in children and young adults. Am J Epidemiol 1994;140:195 – 205.
[7] Boremah CA, Twisk J, Savage MJ, Cran GW, Strain JJ. Phys-ical activity, sports participation, and risk factors in adoles-cents. Med Sci Sports Exerc 1997;29:788 – 93.
[8] Durstine JL, Haskell WL. Effects of exercise on plasma lipids and lipoproteins. Exerc Sport Sci Rev 1994;22:477 – 521. [9] Kujala UM, Ahotupa M, Vasankari T, Kaprio J, Tikkanen
MJ. Low LDL oxidation in veteran endurance athletes. Scand J Med Sci Sports 1996;6:303 – 8.
[10] Vasankari TJ, Kujala UM, Vasankari TM, Ahotupa M. Re-duced oxidized LDL levels after a 10-month exercise program. Med Sci Sports Exerc 1998;30:1496 – 501.
[11] Vasankari TJ, Kujala UM, Vasankari TM, Vuorimaa T, Ahotupa M. Increased serum and LDL antioxidant potential after antioxidant supplementation in endurance athletes. Am J Clin Nutr 1997;65:1052 – 6.
[12] Vasankari TJ, Kujala UM, Vasankari TM, Vuorimaa T, Ahotupa M. Effects of acute prolonged exercise on serum and LDL oxidation and antioxidant defences. Free Radic Biol Med 1997;22:509 – 13.
[13] Ahotupa M, Ruutu M, Mantyla E. Simple methods for quan-tifying oxidation products and antioxidant potential of low density lipoproteins. Clin Biochem 1996;29:139 – 44.
[14] Ainsworth BE, Haskell WL, Leon AS, Jacobs DR Jr, Montoye HJ, Sallis JF, Paffenbarger RS Jr. Compendium of physical activities: classification of energy costs of human physical ac-tivities. Med Sci Sports Exerc 1993;25:71 – 80.
[15] Rastas M, Seppanen R, Knuts L-R, Karvetti R-L, Varo P. Nutrient Composition of Foods. Helsinki, Finland: Publica-tions of the Social Insurance Institution; 1993.
[16] Tanner JM. Growth at Adolescence. Oxford: Blackwell, 1962. [17] Duke PM, Litt IF, Gross RT. Adolescents’ self-assessment for
sexual maturation. Pediatrics 1980;66:918 – 20.
[18] Friedewald WT, Levy R, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma without use of the preparative ultracentrifuge. Clin Chem 1972;18:499 – 502.
[19] Weiland H, Seidel D. A simple specific method for precipita-tion of low density lipoproteins. J Lipid Res 1983;24:904 – 9. [20] Ahotupa M, Marniemi J, Lehtima¨ki T, Talvinen K, Raitakari
OT, Vasankari T, Viikari J, Luoma J, Yla¨-Herttuala S. Base-line diene conjugation in LDL lipids as a direct measure of in vivo LDL oxidation. Clin Biochem 1998;31:257 – 61.
[21] Raitakari OT, Taimela S, Porkka KVK, Telama R, Va¨lima¨ki I, A,kerblom HK, Viikari J. Association between physical activ-ity and risk factors for coronary heart disease: the cardiovascu-lar risk in young Finns study. Med Sci Sports Exerc 1997;29:1055 – 61.
[22] De Graaf J, Hak-Lemmers HLM, Hectors MPG, Demacker PNM, Hendrics JCM, Stalenhoef AFH. Enhanced susceptibil-ity to in vitro oxidation of the dense LDL subfraction in healthy subjects. Arterioscler Thromb 1991;11:298 – 306. [23] Williams PT, Krauss RM, Wood PD, Lindgren FT, Giotas C,
Vranizan KM. Lipoprotein subfractions of runners and seden-tary men. Metabolism 1986;35:45 – 52.
[24] Vasankari T, Fogelholm M, Oja P, Vuori I, Ahotupa M. Ef-fect of weight reduction on LDL oxidation (abstr). Med Sci Sports Exerc 1997;29:S130.
[25] Kujala U, Ahotupa M, Vasankari T, Kaprio J, Tikkanen M. Familial aggregation of LDL oxidation. Scand J Clin Lab In-vest 1997;57:141 – 7.
[26] Steinberg D, Lewis A. Conner Memorial lecture. Oxidative modification of LDL and atherogenesis. Circulation 1997;95:1062 – 71.
[27] Juul K, Nielsen LB, Munkholm K, Stender S, Nordestgaard BG. Oxidation of plasma low-density lipoprotein accelerates its accumulation and degradation in the arterial wall in vivo. Cir-culation 1996;94:1698 – 704.
[28] Berliner JA, Territo MC, Sevanian A, Ramin S, Kim JA, Bamshad B, Esterson M, Fogelman AM. Minimally modified low density lipoprotein stimulates monocyte endothelial inter-actions. J Clin Invest 1990;85:1260 – 6.
[29] Mehta JL, Li DY. Identification and autoregulation of recep-tor for OX-LDL in cultured human coronary artery endothe-lial cells. Biochem Biophys Res Commun 1998;248:511 – 4. [30] Nagase M, Hirose S, Fujita T. Unique repetitive sequence and
unexpected regulation of expression of rat endothelin receptor for oxidized low-density lipoprotein (LOX-1). Biochem J 1998;330:1417 – 22.
[31] Jialal I, Devaraj S. Low-density lipoprotein oxidation, antioxi-dants, and atherosclerosis: a clinical biochemistry perspective. Clin Chem 1996;42:498 – 506.
[32] Esterbauer H, Gebicki J, Puhl H, Jurgens G. The role of lipid peroxidation and antioxidants in oxidative modification of LDL. Free Rad Biol Med 1992;13:341 – 90.
[33] Parks EJ, German JB, Davis PA, Frankel EN, Kappagoda CT, Rutledge JC, Hyson DA, Schneeman BO. Reduced oxidative
susceptibility of LDL from patients participating in an intensive atherosclerosis treatment program. Am J Clin Nutr 1998;68:778 – 85.
[34] Toikka JO, Niemi P, Ahotupa M, Niinikoski H, Viikari JSA, Ronnemaa T, Hartiala JJ, Raitakari O. Large artery elastic properties in young men: relationship to serum lipoproteins and oxidized low-density lipoproteins. Arterioscler Thromb Vasc Biol 1999;19:436 – 41.