Ultrasound determined carotid and femoral atherosclerosis in
Lithuanian and Swedish men: the LiVicordia study
M. Kristenson
a,*, C. Lassvik
b, B. Bergdahl
b, Z. Kucinskie`ne
c, L. Aizienie`ne
d,
Ziede´n Bo
b, Liselotte Scha¨fer Elinder
e, A.G. Olsson
baDepartment of Health and En6ironment,Faculty of Health Sciences,S-58185 Linko¨ping, Sweden bDepartment of Medicine and Care,Faculty of Health Sciences,S-58185 Linko¨ping, Sweden
cDepartment of Physiology and Biochemistry,Medical Faculty,Vilnius, Lithuania dDepartment of Cardiology,Medical Faculty,Vilnius, Lithuania eDepartment of Medicine,Karolinska Institute,Stockholm, Sweden
Received 3 March 1999; received in revised form 8 September 1999; accepted 22 September 1999
Abstract
Coronary heart disease mortality is four times higher in Lithuanian compared to Swedish middle-aged men. Using the same equipment (Acuson XP10 with 5 MHz linear transducer) and staff, we compared the amount of atherosclerosis in carotid and femoral arteries in 100 randomly sampled 50-year-old men in each of the cities Vilnius, Lithuania and Linko¨ping, Sweden. Atherosclerotic plaques were more abundant in Vilnius men compared to Linko¨ping men (53 versus 28% in the common carotid artery, 73 versus 37% in the common femoral artery,PB0.001 for both). Plaques were thicker and more extended in arteries of Vilnius men, and an ultrasound atherosclerosis score was higher in both carotid and femoral arteries (PB0.001 for all). More Vilnius men had a maximal intima-media thickness of the common femoral artery above 1 mm (PB0.005). Stiffness in the common carotid artery was higher in Vilnius men (PB0.001). In a linear regression model of the pooled material, after adjustment for city was made, smoking, systolic blood pressure, low density lipoprotein cholesterol and b-carotene (inversely) significantly contributed to a high total ultrasound score (r2=0.32). These findings show that the higher coronary mortality noted
in Lithuanian men goes together with a higher prevalence of early peripheral atherosclerosis. © 2000 Elsevier Science Ireland Ltd. All rights reserved.
Keywords:Lithuania; Intima-media thickness; Plaque; Stiffness; Risk factors
www.elsevier.com/locate/atherosclerosis
1. Introduction
Mortality trends in coronary heart disease (CHD) are dramatically diverging between Eastern and Western European countries [1 – 3]. For example, the mortality in 1994 among 50 – 54-year-old men due to CHD (ICD-9 codes 410 – 414), was 436 versus 100 per 100 000 inhabitants in Lithuania and Sweden, respectively. The causes for the increasing Eastern European mortality are poorly understood [2,4]. Studies of traditional risk factors for CHD in Lithuania, i.e. serum cholesterol, blood pressure, and smoking, have shown only small
differences in comparison with those in Sweden [5] and The Netherlands [6]. The present Linko¨ping – Vilnius coronary risk assessment study (LiVicordia) has confir-med these results [7]. New findings were that Vilnius men had lower serum concentrations of lipid-soluble antioxidant vitamins and higher susceptibility of low density lipoprotein (LDL) to oxidation than Linko¨ping men.
Vessel wall changes in the carotid and femoral arter-ies have been found to correlate with CHD and have been suggested to serve as surrogate end points or markers for diseased coronary arteries [8 – 11]. Carotid intima-media thickness (IMT) has been related to risk factors for CHD [12 – 14], peripheral atherosclerosis [13,15], and degree of coronary obstruction at angiogra-phy [12]. Presence of atherosclerotic plaques had,
com-* Corresponding author. Tel.: +46-13-225075; fax: + 46-13-225095.
E-mail address:[email protected] (M. Kristenson)
pared to IMT, even stronger relations to acute myocar-dial infarction [9]. Also, an increased arterial stiffness has been suggested to be an indicator of early artery wall disease [16].
The aim of this part of the LiVicordia study was to compare the amount of atherosclerosis in the two pop-ulations by estimating IMT, number and size of atherosclerotic plaques, and wall stiffness. In addition we wanted to relate the findings to traditional and possible new risk factors for CHD.
2. Methods
2.1. Study design
LiVicordia is a cross-sectional study conducted from October l993 to June l994. A list of randomly selected men, born between July 1, l943 and June 30, l944 was obtained from the census register in each of the cities of Vilnius (600 000 inhabitants) and Linko¨ping (130 000 inhabitants). One hundred men in each city underwent an ultrasound investigation of the right carotid and femoral arteries. In Linko¨ping the response rate was
82% and in Vilnius 74%. The only exclusions were two men with serious cancer. The ultrasound examinations were performed between December 1993 and April 1994 in Linko¨ping and during 2 weeks in May 1994 in Vilnius. In Linko¨ping the investigations took place between 10:00 and 12:00 h and in Vilnius between 08:00 and 16:00 h. In addition, anthropometric measures, blood pressure, and blood samples were taken. Details of the procedures and methods for these investigations have been given previously [7]. The study was approved by the Ethical Committee of the Faculty of Health Sciences in Linko¨ping and all participants gave written informed consent.
2.2. Ultrasound measurements and e6aluation
The same Acuson XP10 ultrasound scanner (Acuson, Mountain View, CA) with a 5 MHz linear 2D scanhead was used in both cities, and the same four experienced persons collected primary data. The investigations were standardised according to present recommendations [17,18]. The carotid vessels were investigated for the presence of stenosis with spectral doppler at 60° doppler angle, and if a peak systolic velocity of more
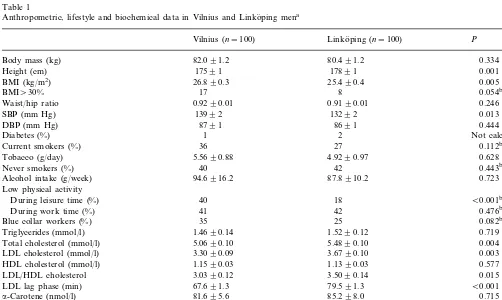
Table 1
Anthropometric, lifestyle and biochemical data in Vilnius and Linko¨ping mena
Vilnius (n=100) Linko¨ping (n=100) P
82.091.2
Body mass (kg) 80.491.2 0.334
Height (cm) 17591 17891 0.001
26.890.3
BMI (kg/m2) 25.490.4 0.005
17
BMI\30% 8 0.054b
0.9290.01
Waist/hip ratio 0.9190.01 0.246
13992 13292
SBP (mm Hg) 0.013
8791 8691
DBP (mm Hg) 0.444
Not calculated 2
Diabetes (%) 1
0.112b
36
Current smokers (%) 27
Tobacco (g/day) 5.5690.88 4.9290.97 0.628
42 0.443b
40 Never smokers (%)
0.723 94.6916.2
Alcohol intake (g/week) 87.8910.2
Low physical activity
During leisure time (%) 40 18 B0.001b
0.476b
42
During work time (%) 41
35
Blue collar workers (%) 25 0.082b
Triglycerides (mmol/l) 1.4690.14 1.5290.12 0.719
0.004 Total cholesterol (mmol/l) 5.0690.10 5.4890.10
3.3090.09
LDL cholesterol (mmol/l) 3.6790.10 0.003
HDL cholesterol (mmol/l) 1.1590.03 1.1390.03 0.577
LDL/HDL cholesterol 3.0390.12 3.5090.14 0.015
67.691.3
LDL lag phase (min) 79.591.3 B0.001
0.715
81.695.6 85.298.0
a-Carotene (nmol/l)
512933 0.001
377920 b-Carotene (nmol/l)
Lycopene (nmol/l) 316922 617933 B0.001
3.390.1 3.490.1 0.345
a-Tocopherol (mmol/mmol)c
0.2590.01 0.4690.02
g-Tocopherol (mmol/mmol)c B0.001
ameans9SEM, BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; HDL, high density lipoprotein; LDL, low
density lipoprotein.
bChi-square test.
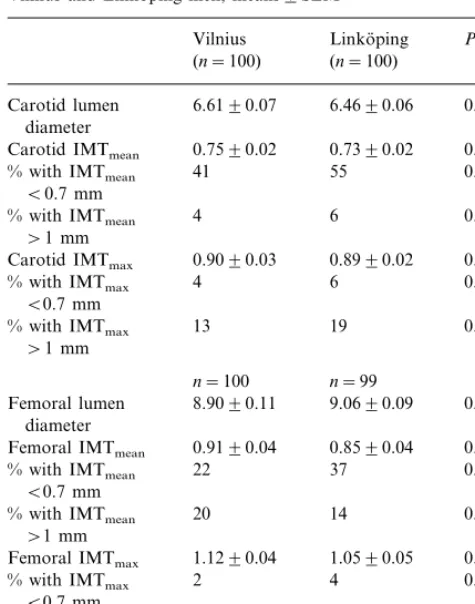
Table 2
Lumen diameter, mean and maximal intima-media thickness (IMTmean, IMTmax) in mm and % of men with IMTmean and
IMTmaxB0.7 and\1 mm in the carotid and femoral arteries of
Vilnius and Linko¨ping men, means9SEM
Linko¨ping
Vilnius P
(n=100) (n=100)
6.6190.07
Carotid lumen 6.4690.06 0.117
diameter
0.7390.02
Carotid IMTmean 0.7590.02 0.148a
% with IMTmean 41 55 0.048b
B0.7 mm
% with IMTmean 4 6 0.516b
\1 mm
0.8990.02
Carotid IMTmax 0.929
a
Femoral lumen 8.9090.11 9.0690.09 0.255 diameter
0.8590.04
Femoral IMTmean 0.005
a
aMann–Whitney’sU-test. bChi-square test. cFisher’s exact test.
an ankle cuff and an ultrasound Doppler probe on the posterior tibial artery.
Two researchers performed off-line evaluations of all data from both centres using a computerised analysing system [19] permitting about 100 paired measurements at 10 mm. The mean of three different images of the same segment was used in the calculations, resulting in about 300 paired measurements in each volunteer. Lu-men diameter was defined as the mean distance between leading edges of the proximal and distal lumen-intima interfaces and the IM-complex as the mean and maxi-mal distance between distal lumen-intima and media-adventitia interfaces (IMTmean, IMTmax). In both CCA and CFA, lumen diameter, IMTmean, IMTmax and wall movements (systolic minus diastolic diameter, in CCA only) were measured in a 10 mm long section immedi-ately adjacent to the bifurcation. A plaque was defined as a distinct area with an IMT more than 50% thicker than neighbouring sites, if the IM-complex was visible in that projection. In the CCA, carotid bulb and CFA this was usually so, but in the carotid bifurcation small echogenic plaques were often found in the lateral or anterior walls. These were also included and measured but with less accuracy, as the IM-complex could not be exactly delineated. In some cases with large plaques in the CFA no exact delineation could be made in the cranial direction, so the proximal limit of the plaque was set where the external iliac artery ‘descends down’ into the bowel. Plaques were recorded both in the longitudinal and in the transverse mode. Plaque size was evaluated by maximal height and area, only in a longitudinal image. Delineation of plaque was con-ducted visually. Arterial stiffness in CCA was calcu-lated as b=log (systolic/diastolic arm BP) divided by (wall movement /diastolic diameter) [16,20].
All tapes were measured in random order with regard to city of origin. Reproducibility of double recordings for the laboratory has been measured in patients with hyperlipidemia. The results are expressed as the per-centage difference, i.e. the difference between highest and lowest value divided by lowest value (×100), and were in CCA and CFA, respectively: lumen diameter 494% and 593%, IMTmax 1098% and 15914%, IMTmean 898% and 14910%; plaque height 1198% and 795%, plaque area 13910% and 13912%, and stiffness 14911% (CCA only).
An ultrasound atherosclerotic score (UAS) was cal-culated from IMTmax and/or the largest plaque in each of CCA and CFA as follows: IMT51 mm and no plaque was considered normal=0 points; IMTB1 – 2 mm or a plaque with a maximal height of 1 mm (only present in the carotid bifurcation)=2 points; a plaque with maximal height of \1 – 2 mm=4 points; maximal height \2 mm=6 points; 50% stenosis=8 points; and high grade stenosis\70% or occlusion=10 points. than 1.2 m/s was found in conjunction with a plaque,
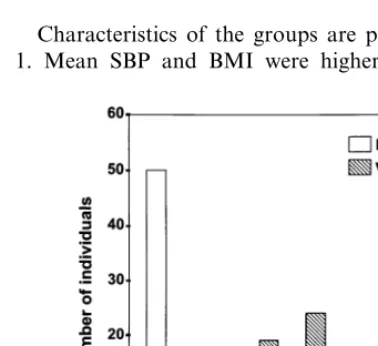
Table 3
Percentage of men with plaques, maximal height and longitudinal area of plaque,% of men with plaque height and areas above specified values and ultrasound score (UAS) in the bifurcational area of the common carotid (CCA) and femoral (CFA) arteries, means 9SEM
Linko¨ping (n=100) P Vilnius (n=100)
CCA
28
53 B0.001b
% Of men with plaque
0.4890.1
height (mm) 0.8390.1 0.001a
20
32 0.053b
% of men with plaque height\1 mm
9 0.489b
% of men with plaque height\2 mm 12
3.2990.88
5.8491.2 0.001a
area (mm2)
30
% of men with plaque area\5 mm2 17 0.030b
10
% of men with plaque area\15 mm2 5 0.179b
CFA
% Of men with plaque 73 37 B0.001b
0.7790.1
1.5090.1 B0.001a
height (mm)
32
% of men with plaque height\1 mm 65 B0.001b
16
33 0.005b
% of men with plaque height\2 mm
area (mm2) 15.891.8 9.0291.7 B0.001a
29
55 B0.001b
% of men with plaque area\8 mm2
18
% of men with plaque area\22 mm2 25 0.115b
50
85 B0.001b
% with plaque in one or both arteries
1.1490.20
Carotid UAS (points) 1.9490.22 0.002
1.7090.24
3.4290.24 B0.001
Femoral UAS (points)
2.8490.35
Total UAS (points) 5.3590.35 B0.001
aMann-Whitneys test. bChi-square test.
2.3. Biochemical analysis
Samples for plasma lipoprotein analysis were drawn in the fasting state. LDL was determined according to the Friedewald formula [21]. The susceptibility of LDL to oxidation was measured as described by Kleinfeld et al. [22]. Plasma concentrations of the lipophilic antioxi-dant vitamins a- and g-tocopherol and a- and b -carotene were determined by reverse phase high performance liquid chromatography [23]. Concentra-tions of a- and g-tocopherol were expressed per total triglyceride plus total cholesterol concentrations.
2.4. Statistical methods
The distribution of measures of intima media and of area and height of plaques were skewed, and therefore the Mann – Whitney’s test (two-tailed) was used to test differences between the two groups. For continuous, normally distributed data Student’s t-test, and for di-chotomous variables chi-square test were used. Linear multiple regression models were used to analyse the dependence of IMTmean, IMTmax, UAS, and stiffness on SBP, smoking and LDL-cholesterol, a- and g- toco-pherol, a- and b-carotene, lycopene, and lag phase for oxidation of LDL. In these models, interactions be-tween city and the independent variables were tested and found not to be significant. Therefore, we present results from regression models for pooled data. Only adjusted explanatory values (r2) are presented. Partial
correlation analyses, adjusted for city, were performed to analyse the associations between the independent variables and for relationships between the different ultrasound measures used. A P-value of 0.01 or less was regarded as significant.
3. Results
Characteristics of the groups are presented in Table 1. Mean SBP and BMI were higher in Vilnius men,
Table 4
Stiffness and wall motion in the common carotid artery (CCA), systolic blood pressure (SBP), diastolic blood pressure (DBP), pulse pressure and ankle-brachial index, means 9SEM
Linko¨ping
tively), but pulse pressure did not differ. Also, ankle-brachial index (i.e. ankle systolic pressure/arm systolic pressure) did not differ between the cities (Table 4).
The correlation analysis between the independent variables included in the linear regression models showed, after adjustment for city, significant and high correlations (range 0.75 – 0.77) between SBP and DBP, and betweena-carotene andb-carotene. Moderate, and significant correlations (range 0.21 – 0.37) were found for botha-andb-carotene to lycopene, LDL-cholesterol and to a-tocopherol. Likewise, moderate correlations were found between a-tocopherol and lag phase, and (negative) between smoking and a-carotene.
The linear regression model for total UAS is pre-sented in Table 5. In a multiple stepwise model on the pooled patient sample from both cities, in which city was first entered into the model, smoking, high SBP, high LDL-cholesterol, and low b-carotene significantly contributed to high total UAS (r2=0.32). In models for the two cities taken separately, the explanatory value was higher for Linko¨ping men than for Vilnius men (r2=0.37 and 0.14, respectively). In the Linko¨ping group, smoking, high LDL cholesterol, lowb-carotene, and high a-tocopherol significantly related to a high total UAS; in Vilnius this was the case for smoking, high SBP, and low lycopene. When the multiple step-wise model was used for the carotid UAS separately, on the pooled patient sample, in which city was first en-tered, high SBP, DBP, smoking and high a-tocopherol came out significantly (r2=0.18). For femoral UAS smoking, high LDL, and low b-carotene significantly contributed (r2=0.29). Linear regression models with IMT as the dependent variable and controlled for city, showed low explanatory values (carotid IMT;r2=0.08 and femoral IMT; r2=0.15). SBP contributed signifi-cantly to high carotid IMT; smoking and LDL-choles-terol to high femoral IMT, the results being the same for IMTmean and IMTmax values. In the model with stiffness as dependent variable, high SBP significantly contributed to high carotid stiffness (r2
=0.18). Neither BMI, low physical activity, a-carotene, g-tocopherol nor LDL lag phase contributed significantly to amount of atherosclerosis in any of the models tested.
total and LDL cholesterol were higher in Linko¨ping men while smoking habits, alcohol intake and diabetes prevalence were similar in the two cities. More Vilnius men reported low physical activity at leisure time, but there was no difference in the proportion of men with low physical activity at work time. Serum levels of the lipid soluble antioxidant vitamins b-carotene, lycopene andg-tocopherol were lower and mean LDL lag phase shorter in Vilnius than in Linko¨ping men.
Measures of lumen diameter and IM-complex were obtained in all but one individual with an extensive femoral plaque. Results are presented in Table 2. In the CFA, a larger proportion of Vilnius men had IMTmax above 1 mm (P=0.005). In CCA no significant differ-ences for these measures were found. Mean lumen diameter did not differ in either artery. As shown in Table 3, plaques were more common in Vilnius men, both in CCA and in CFA (PB0.001 for both). Also, more Vilnius men had, in both CCA and CFA, larger plaques, both measured as height and area (PB0.001 for all). Accordingly, their CCA, CFA and total UAS were higher (Fig. 1). Flow velocity was normal in all investigated arteries. Wall movement in CCA was lower and calculated stiffness in CCA higher in Vilnius men (P for bothB0.001). Both SBP and DBP, measured just after registration of vessel wall motility, were higher in Vilnius men (P=0.002 andPB0.001,
respec-Table 5
Multiple linear regression analysis with total ultrasound atherosclerosis score as dependent variable, pooled group,n=200a
P Standard error of Beta
Partial regression coefficient
Country 2.178 0.499 B0.001
Tobacco (g/day) 0.148 0.028 B0.001
0.030 0.012 0.013
SBP (mm Hg)
LDL cholesterol (mmol/l) 0.920 0.264 0.001
−0.003 0.001 0.004
b-carotene (nmol/l)
4. Discussion
To our knowledge, the present study is the first to show results from comparisons of ultrasound investiga-tions of peripheral arteries in random populainvestiga-tions in Eastern and Western Europe. We found that Vilnius men, representing a population with a fourfold higher CHD mortality compared to Linko¨ping men, had clear signs of more advanced atherosclerosis on several measures.
A limitation of the study is the relatively small sam-ple size. However, we used a random samsam-ple from the strata of 50-year-old men which gave a high representa-tivity. Also, the study was carefully standardised and had a high response rate.
The relevance of IMT measures to study CHD has been questioned, because only weak associations to findings on coronary angiograms have been found [24]. However, in large prospective studies, the risk of CHD was increased about twofold in individuals with in-creased carotid IMT compared to individuals without [9,11], and fourfold for men with plaques compared to men without [9]. As atherosclerosis is a focal disease, making ultrasound measurements at several arterial sites is to be recommended. As in previous studies [8,14], we made a search for plaques in both the carotid and the femoral arteries. Examining both sides has also been recommended [25], but like other researchers [14], we only evaluated the right side for feasibility reasons. The presence of large plaques in the CFA caused difficulty in delineating the IM-complex, and it can be argued that an increase in IMT might be part of an adjacent plaque in some cases. Therefore, in the regres-sion models we used an ultrasound score that included both IMT and plaque. This seems logical, as an in-crease of IMT and the evolution of plaques may be part of the same process, and this model has been used previously [8].
The use of a standard 5 MHz linear transducer might have caused a slight measurement error due to lower image resolution than can be achieved by a broadband transducer. However, our reproducibility of measure-ments was similar to that of other groups [9,18,26] and in an earlier study no difference was found in measure-ments with both modalities [19]. Similarly, the use of M-mode to determine wall stiffness may be considered inadequate due to less resolution than echo-tracking. Again, reproducibility of these measurements was shown to be similar [27]. Mean values of carotid IMTmaxwere in the same range as found in 48 – 54-year-old men in Eastern Finland (0.84 – 0.98 mm) [28]. Com-pared to several other study groups [8,9,29], plaques were more common in Vilnius men. Stiffness was also higher in CCA of Vilnius compared to Linko¨ping men. Our results on stiffness are in the same range with findings in male subjects from normal populations in
corresponding age groups [30]. In other studies atherosclerosis in the femoral artery appears to be more advanced or to develop earlier, compared to the carotid artery [8,14]. Our findings are in line with this experience.
In the regression model for total UAS, we found smoking, LDL cholesterol and SBP to be significant predictors. In the majority of published reports, risk factors have been related to carotid IMT, with LDL cholesterol, SBP and smoking emerging as the most important predictors [9,14,31,32]. A different risk profile for CCA and CFA has also been described [9]. As in our study, LDL cholesterol has been found to be important for femoral atherosclerosis [33].
The traditional risk factors for CHD and antioxidant vitamins explained only a minor part of the difference in UAS between men from the two cities, and lipid levels had the opposite effect; LDL cholesterol levels were lower in Vilnius men, i.e. in the sample from a population with a higher CHD mortality. However, both cities belong to populations with mean cholesterol levels which are high by international standards, and therefore both populations have a high susceptibility to CHD [3].
In Vilnius men traditional risk factors contributed less to total UAS than in Linko¨ping men. One explana-tion may be that these factors have less explanatory power to predict CHD in low as compared to high socioeconomic populations [34,35]. There were small differences in the proportion of blue collar men be-tween Vilnius and Linko¨ping. However, large differ-ences in the socioeconomic situation between the cities are evident. We also found unfavourable characteristics in a range of psychosocial risk factors for CHD among Vilnius men as compared to Linko¨ping men [36,37]. Still, these factors did not help explain differences between the cities in UAS score. Yet unknown risk factors seem to play an important role in explaining atherosclerosis, especially in Lithuanian men.
low atherogenic score is that b-carotene serves as a marker for a high intake of green and yellow vegeta-bles. These foods have been shown to protect against CHD [43] and have been suggested to have important implications for cardiovascular health in Eastern Eu-rope [44,45].
In conclusion, our findings show that the observed difference in CHD between Sweden and Lithuania goes together with a higher prevalence of early atherosclero-sis in Lithuanian men. Antioxidant status may play a role in this development.
Acknowledgements
This study was supported by grants from the Swedish Medical Research Council no 6962, The Royal Swedish Academy of Sciences, the Swedish Institute, Linko¨ping University, Procordia Research Fund and A, ke Wiberg’s Fund. We thank nurses Susanne Wa¨rjerstam-Elf, Regina Milasiene´ and Grazina Martinaitiene, assis-tants Snaige Jermaliene´, Eva Fa¨rm, Camilla Nilsson and Britt-Marie Gustavsson, biomedical analysts Siv-Britt Babtist, Siv-Britt Sigfridsson and Ylva Svensson for skilful technical assistance, PhD Carin Kullberg for help with statistical analyses, and Professor John Carstensen for advice on statistical interpretation.
References
[1] Feachem R. Health decline in Eastern Europe, Nature 1994;367:313 – 314.
[2] UNICEF. Crises in mortality, health and nutrition, Florence, 1994.
[3] WHO. Health for all database, Copenhagen, 1991.
[4] Bobak M, Marmot M. East – West mortality divide and its potential explanations: Proposed research agenda, Br Med J 1996;312:421 – 425.
[5] Pajak A, Kuulasmaa K, Tuomilehto J, Ruokokoski E. Geo-graphical variation in the major risk factors of coronary heart disease in men and women aged 35 – 64 years. The WHO MON-ICA project, World Health Stat Q 1988;41:115 – 139.
[6] Bosma H, Appels A, Sturmans F, Grabauskas V, Gostautas A. Differences in mortality and coronary heart disease between Lithuania and the Netherlands: Results from the WHO Kaunas-Rotterdam intervention study (KRIS), Int J Epidemiol 1994;23:12 – 19.
[7] Kristenson M, Ziede´n B, Kucinskiene Z, Scha¨fer-Elinder L, Bergdahl B, Elwing B, et al. Antioxidant state and mortality from coronary heart disease in Lithuanian and Swedish men: concomitant cross sectional study of men aged 50, Br Med J 1997;314:629 – 633.
[8] Belcaro G, Fisher C, Veller M, Renton S, Geroulakos G, Ravasmani G, et al. Screening asymptomatic subjects with sub-clinical arteriosclerotic lesions with arterial ultrasonic biopsy. The P.A.P. study. VASA 1993;22:232 – 240.
[9] Salonen JT, Salonen R. Ultrasound B-mode imaging in observa-tional studies of atherosclerotic progression, Circulation 1993;87(supplement II); 56 – 66.
[10] Crouse JR, Thompson CJ. An evaluation of methods for imag-ing and quantifyimag-ing coronary and carotid lumen stenosis and atherosclerosis, Circulation 1993;87(supplement II):17 – 33. [11] Chamberless LE, Heiss G, Folsom AR, Rosamond W, Szklo M,
Sharrett AR, et al. Association of coronary heart disease inci-dence with carotid arterial wall thickness and major risk factors: The atherosclerosis risk in communites (ARIC) study, 1987 – 1993, Am J Epidemiol 1997;146:483 – 494.
[12] Geroulakos G, O’Gorman DJ, Kalodiki E, Sheridan DJ, Nico-laides AN. The carotid intima-media thickness as a marker of the presence of severe symptomatic coronary heart disease, Eur Heart J 1994;15:781 – 785.
[13] Grobbee DE, Bots ML. Carotid artery intima-media thickness as an indicator of generalised atherosclerosis, J Intern Med 1994;236:567 – 573.
[14] Wendelhag I, Wiklund O, Wikstrand J. Atherosclerotic changes in the femoral arteries in familial hypercholesterolemia. Ultra-sonografic assessment of intima-media thickness and plaque occurrence, Arterioscler Thromb Vasc Biol 1993;13:1404 – 1411. [15] Bots ML, Hofman A, Grobbee DE. Common carotid intima-media thickness and lower extremity arterial atherosclerosis, Arterioscler Thromb Vasc Biol 1994;14:1885 – 1891.
[16] Arnett DK, Evans GW, Ward AR. Arterial stiffness: A new cardiovascular risk factor? Am J Epidemiol 1994;140:669 – 682. [17] Wikstrand J, Wendelhag I. Methodological considerations of
ultrasound investigation of intima-media thickness and lumen diameter, J Intern Med 1994;236:555 – 559.
[18] Persson J, Stavenow L, Wikstrand J, Israelsson B, Formgren J, Berglund G. Noninvasive quantification of atherosclerotic le-sions. Reproducibility of ultrasonographic measurement of arte-rial wall thickness and plaque size, Arterioscler Thromb Vasc Biol 1992;12:261 – 266.
[19] Wendelhag I, Wiklund O, Wikstrand J. On quantifying plaque size and intima-media thickness in carotid and femoral arteries, Arterioscler Thromb Vasc Biol 1996;16:843 – 850.
[20] Buntin CM, Silver FH. Noninvasive assessment of mechanical properties of peripheral arteries, Ann Biomed Eng 1990;18:549 – 566.
[21] Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge, Clin Chem 1972;18:499 – 502.
[22] Kleinveld HA, Hak-Lemmers HL, Stalenhoef AFH, Demacker PNM. Improved measurement of low-density-lipoprotein suscep-tibility to copper-induced oxidation: Application of a short procedure for isolating low-density lipoprotein, Clin Chem 1992;38:2066 – 2072.
[23] Scha¨fer Elinder L, Walldius G. Simultaneous measurement of serum probucol and lipid-soluble antioxidants, J Lip Res 1992;33:131 – 137.
[24] Adams M R, Nakagomi A, Keech A, Robinson J, McCredie R, Bailey BP, et al. Carotid intima-media thickness is only weakly correlated with the extent and severety of coronary artery dis-ease, Circulation 1995;92:2127 – 2134.
[25] Howard G, Burke GL, Evans GW, Crouse III JR, Riley W, Arnett D, et al. Relations of intimal-medial thickness among sites within the carotid artery as evaluated by B – mode ultra-sound, Stroke 1994;25:1581 – 1587.
[26] Kanters SD, Algra A, van Leeuwen MS, Banga JD. Reproduci-bility of in vivo carotid intima-media thickness measurements, Stroke 1997;28:665 – 671.
[27] Jensen-Urstad K, Rosfors S. A methodological study of arterial wall function using ultrasound technique, Clin Physiol 1997;17:557 – 567.
[29] Li R, Duncan BB, Metcalf PA, Crouse III JR, Sharrett AR, Tyroler HA, et al. B-mode-detected carotid artery plaque in a general population. Atherosclerosis Risk in Communities/ (ARIC)/Study Investigators, Stroke 1994;25:2377 – 2383. [30] Jonasson T, Henrikssen E, Kangro T, Nilsson H, Vessby B,
Ringqvist I. Stiffness of the common carotid artery in healthy 50-year-old subjects, Clin Physiol 1997;17:569 – 577.
[31] Geroulakos G, O’Gorman D, Nicolaides A, Sheridan D, Elkeles R, Shaper AG. Carotid intima-media thickness: Correlation with the British Regional Heart Study risk score, J Intern Med 1994;235:431 – 433.
[32] Persson J, Formgren J, Israelsson B, Berglund G. Ultrasound-determined intima-media thickness and atherosclerosis. Direct and indirect validation, Arterioscler. Thromb Vasc Biol 1993;14:261 – 264.
[33] Mo¨lgaard J, von Schenck H, Kuusi T, Holme I, Lassvik C, Taskinen M.-R, et al. Plasma lipoprotein abnormalities and apolipoprotein E phenotypes in intermittent claudication. A multivariate analysis of randomly selected subjects, Nutr. Metab Cardiovasc Dis 1996;6:114 – 123.
[34] Blaxter M. Health and lifestyle. London: Routledge, 1990. [35] Hein HO, Suadicani P, Gyntelberg F. Ischemic heart disease
incidence by social class and form of smoking: the Copenhagen male study — 17 years follow-up, J Intern Med 1992;231:477 – 483.
[36] Kristenson M, Kucinskiene Z, Bergdahl B, Calcauskas H, Ur-monas V, Orth-Gomer K, Increased psychosocial strain in Lithuanian versus Swedish men: The LiVicordia study, Psycho-som Med 1998;60:277 – 282
[37] Kristenson M, Orth-Gomer K, Kucinskiene Z, Bergdahl B, Calcauskas H, Balinkiene I, Olsson A. Attenuated cortisol re-sponse to a standardised stress test in Lithuanian versus Swedish men: The LiVicordia study, Int J Behav Med 1998;5:17 – 30. [38] Steinberg D, Parthasarathy S, Carew TE, Khoo JC, Witztum JL.
Beyond cholesterol. Modifications of low-density lipoprotein that increase its atherogenicity, N Engl J Med 1989;320:915 – 924. [39] Kardinaal AFM, Kok FJ, Ringstad J, Gomez-Aracena J, Mazaev VP, Kohlmeier L, et al. Antioxidants in adipose tissue and risk of myocardial infarction: the EURAMIC study, Lancet 1993;342:1379 – 1384.
[40] O8hrvall M, Sundlo¨f G, Vessby B. Gamma, but not alpha tocho-pherol levels in serum are reduced in coronary heart disease patients, J Intern Med 1996;239:111-117.
[41] Riemersma RA, Wood DA, Macintyre CCA, Elton RA, Gey KF, Oliver MF. Risk of angina pectoris and plasma concentra-tions of vitamins A, C, and E and carotene, Lancet 1991;337:1 – 5.
[42] Bowry W, Ingold KU, Stocker R. Vitamin E in human low-den-sity lipoprotein. When and how this antioxidant becomes a pro-oxidant, Biochem J 1992;288:341 – 344.
[43] Gaziano JM. Antioxidant vitamins and cardiovascular disease, Proc Assoc Am Physicians 1999; 111: 2 – 9.
[44] Ginter E. Cardiovascular risk factors in the former communist countries. Analysis of 40 European MONICA populations, Eur J Epidemiol 1995; 11:199 – 207.
[45] Zatonsky WA, McMichael AJ, Powles JW. Ecological study of reasons for the sharp decline in mortality from ischemic heart disease in Poland since 1991, Br Med J 1998; 316: 1047 – 1051.