42
Madiyono et al. Med J IndonesCtinical
Features
and
Management
of
Secundum
Atrial
Septal Defect
in
Infants
and
Children
Bambang
Madiyono,
Jumiety Achmad, Sudigdo
Sastroasmoro,Ismet
N.
Oesman, SukmanTulus
PutraAbstrak
Dalan penelitian retrospekûfini dilakukan evaluasi terhadap penampilan Hinis dan tata laksana pasien defek septum atriun yang berobat di Subbagian Kardiologi, Bagian llnw Kesehatan Anak RS. Cipto Mangunkusunto, Jakarta, antara
I
Januari 1983 sanpai dengan 3 1 Desember 1992. Sebelun tersedia alat ekokardiografi, diagnosis defek septwn atriurn sernata-nata didasarkan pada riwayat penyakit, petneriksaanfisis, elektrokardiogram, danfoto rontgen dada- Setelah tersedia alnt ekokardiografi (Januari 1987), diagnosis kelainan ini dipastikan dengan ekokardiografi (keuudianjuga Doppler dan Doppler berwarna). Seri ini nenunjukkan: (1) Defekseptunt atriun sekundun lebih sering ditenukan pada anak perentpuan, dengan rasio perentpuan : lelaki:
1,5: 1,2; (2) Jwnlah pasien yang
didiagnosis sebagai defek septurn atrium lebih banyak setelah tersedia alat ekol<ardiografi;(i)
Penemuan klinis dan pemerilcsaan prnuÀiong yang khas lebih sering didapatlan pada pasien berusia 3 tahun atau lebih dibanding dengan yang berusia kurang dari 3tahun; (4) Hantbatan pertu,ilbuhan, Icardionegali, dan right branch block lebih sering ditenmkan pada defek besar; (5) Pengobatan terpilih adalah operasi penutuPan defek, yang dapat dilakukan tiap
saat-Abstract
This retrospective study aitned to review the clinicalfeatures and nanagement o;fpatients with secunduu atrial septal defect (ASD 2")- The subjecrs studied were 9O boys (39.8%) and 136 girls (60.2%), treated at the Ourpatient Clinic, Cardiology Division, Deparrnent of Child Health, Cipto Mangunkusumo Hospital, Jakarta, Indonesia, frotn January 1, 1983 to December 31, 1992. Clinical ossessilrcnt and nnnagetnent were evaluated by one ofthe authors. Electrocardiographic, radiographic, and henodynanùc findings were analyzed b), the etperîs. The diagnostic procedure was contpleted u'ith echocardiographic exanination since January 1987. This study discloses severalfindings: (1)ASD20 affectedgirls ntorethanboys, the sex ratiowas 1,5:1; (2)The diagnosis ofASD 2" in infants was increased after the advent of echocardiographl,;
p)
While rypical auscultatory findings could be heard in older ASD ccrses, the clinical features were not specirtc in young infunts; (4) Growth retardation, cardiouegaly and right bundle branch block were couttttonin
large ASD2";
(5) Simple closure ofASD 2" was the procedure ofchoice.Key w ords : at r i al s ep tal defe ct, e cho car d i o gr aphy, c Ii ni c al n anife stat i o ns
Secundum
atrial
septaldefect
(ASD
2)
is
thethird
or
second heartsound
andsoft
eiection
systolic mutmur
at
the upper
left
sternal
bordËr.a'6'7In
young
infants
nical findings are usually
notographic examination
isusually
diagnosis.l3-16
The purpose
of this
study
wasto review
thephysical
as well
as electrocardiographic, radiographic,
andechocardiographic
findings of
patients
with ASD
2otreated
at our
Outpatient
Pediatric Cardiology
Clinic
during
thelast l0
years.METHODS
This retrospective
studyreviewed
theclinical findings
and management of patientswith
ASD
2() treated at theOutpatient
Clinic,
Cardiology
Division,
Departmentof
Child Health, Cipto Mangunkusumo Hospital,
Jakarta,lourth
most common congenrtal neart olsease ln
childhood,
accounting
for
approximalely
7. percentof
all children with
congenital
heartdisease.'-' Most
in-fantswith
this defect are asymptomatic, and frequentlytheir
condition
goes undetecteduntil
school age.Most
patientswith
a moderateleft-to-right
usually complain
only
of mild fatigue
anddyspnea.*
The frequency
of
fatigue and
dyspnea increases
in
infants
with
largeshunt,
andcardiac
failure
occasionally
o""*r.5
ASD 2" is easily
recognized
in older
patients
by
thetypical auscultatory findings consisting
ofwidely
fixed
fourth
congenital
heart disease in
Depart,nent of
Child
Health, Medical School, Universiq,sf
Indonesia, Jakarra, IndonesiaVoI 5, No 1, January - March 1996
Indonesia,
from
January
l,
1983
to
December
31, 1992.Before
echocardiographic machine
was available in
our department,
the diagnosis
of
ASD was
based ontypical
clinical
symptoms and signs,
electrocar-diogram,
and chestX-ray examinations.
Since January 1, 1987,when electrocardiograhic machine
wasavail-able,
the diagnosis was confirnred
by
echocar-diographic examination.
Cardiac catheterization
wasonly performed
oncertain indications
prior
tosurgical
closure.Suggestive
diagnosis
of
ASD
by
the referring
physicians was noted.
Clinical
symptoms
such
asrecurrent respiratory
tract
infections (more than
4 episodes per year), easyfatigability
(as reportedby
the parents), dyspneaon exertion,
andgrowth retardation
(weight
per
age,
NCHS
standard) were
recorded. Physicalexamination
wasthoroughly
carried out by anexperienced
staff. Signs
of
typical
auscultatory
find-ings of ASD
2o,i.e.,
widely fixed
second heart sound andejection systolic murmur
were noted by oneof
the authors.Complete
electrocardiogram
was recordedin all
cases, i.e., standard leads,unipolar
limb
leads and chest leadsV3R, V1-V6.
All electrocardiograhic tracings
werereviewed
and assessedby
theauthors. Heart size
wasevaluated
roentgenographycally
by
measuring
thecardio-thoracic ratio, i.e., the ratio
of
the
maximum
width
of
the heart to thebody thorax
at thelevel of
theright diaphragm
inantero-posterior view. M-mode
andtwo
dimensional echocardiograms were performed
in
all patients
seenafter January
l,
1987using
ALOKA
SSD
720.
The
echocardiographic examination
wascompleted
by color Doppler
echocardiography using
ALOKA
SSD
870.
Cardiac catheterization was
per-formed
prior to
surgery
in
some special
caseswith
suggestivepulmonary hypertension.
The
patients were
arbitrarily divided into two
groups; GroupA
consistedof
patientsadmitted during
thefirst
four-year period (from
January
l,
19g3to
December31,
1986),where echocardiography
was notavailable,
while
Group B comprised
the restof
patientsadmitted
afterward.
For statistical analysis
numerical results
aregiven
asmean (standard
deviation
of
the nrean).
euantitative
data were
comparedby Student's t A
valueof
p < 0,05 was consideredstatistically significant.
Atrial Septal
Defect
43RESULTS
Two
hundred andtwenty six patients
wereenrolled in
the study.
They were
90 boys
(39.8To)and
136girls
(60.2%). The female
to maleratio
thusbeing
1.5:1, soASD
20affected
girls
more than boys
asis generally
the case. l-4The diagnosis
of ASD
hadalready
been suggestedby
the referring physicians
in 62
cases(27.4%), most
of
them
aged 3 yearsor more.
This relatively small
per-centageindicates
thatASD
2ocould
berecognized by
thereferring physicians
in
someolder
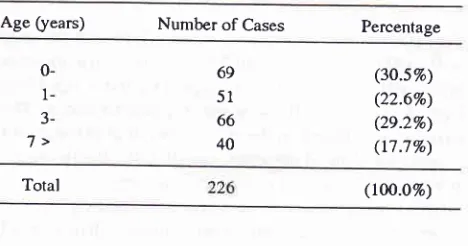
cases.The distribution
of
patients studied
basedon the
agegroup at the
first
evaluation showed
binrodal
pattern(Table
1), thetwo
peakswere
at the agegroup
of
lessthan
I
year (3O.57o) and3-6
years(29.2%),
respective-ly.
Table 1. Sex and age distribution of 226 ASD 20 patients
Age (years) Number of Cases Percentage
0-
l-
3-7>
69
5l
66 40
(3o.s%) (22.6%) (2e2%) (t7.7%)
Total (too.o%)
Table
2
depicts the number of patients
by
age, based on 5year-period of study. It
is clear that the numberof
patientswith ASD
2o increasedin
the last 5 years (144 casesor
25 cases per year), comparedwith
thenumber
ofpatients in
the second 5-yearperiod
(g2 patients,or
17
casesper year).
This
table also shows that
theproportion
of
ASD
patients less than 3 years
of
ageincreased
from
41.5%
in the
first
5-year period to
59.7%in
the second5-year period.
Table
2. Age
distributionof
226 patients basedon
5_year period of diagnosisAge
(years) 1983-1987
lgïB-tgg2
<3
3 or more34 (4t.s%) 48 (58.57o')
86
(s9.77o)
t2O (53.5Vo) s8(40.3%)
106 (46.s%) [image:2.595.296.530.358.481.2]-I
44
Madiyono et al.Further interesting result
is seenif
the agedistribution
of
patients studied
was relatedwith
theavailability
of
echocardiographic machine.
The number
of
patients
with ASD
2oin this
series was increasedsignificantly,
i.e.,49
patients
in
thefirst
4years (12
casesper
year)compared
with
177patients
in
the
last
six
years
(30 [image:3.595.51.287.264.350.2]cases
per
year).
SeeTable 3. The
proportion of ASD
patients
diagnosedbefore
the ageof
3 years increasedfrom28.6% during
1983-1986 to
ashigh
as599% in
theperiod
of
1987-1992.
Table 3. Age distribution of 226 patients based on echocardio-graphic availability
Med J Indones
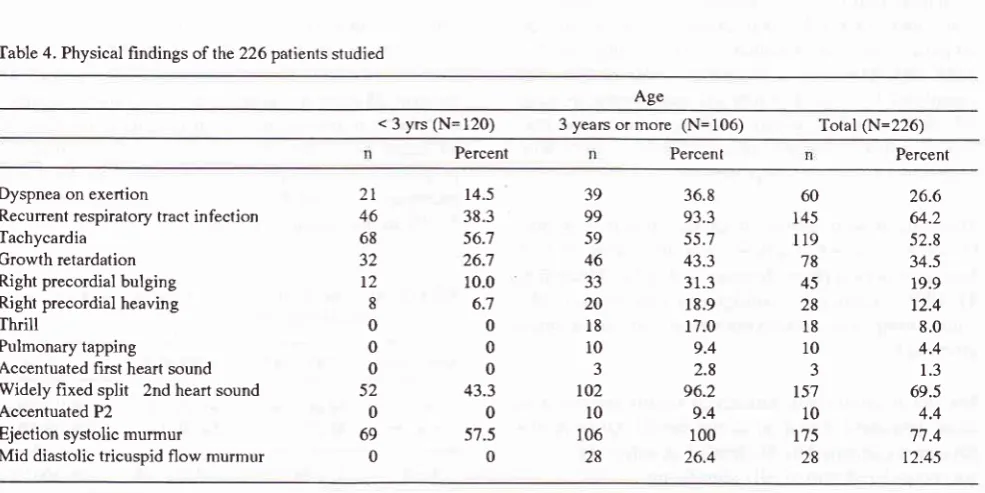
patients aged less than 3 years.
Marked differences
wasfound
in
dyspnea
on
exertion (36.8%
in
group
of
patients
3
years
old or
more
vs
15.57oin
group
of
patients
lessthan
3years),
growth
retardation
(43.37ov s 26.7 %),
palpable
thrill
(L7 .O7o v s O%),widely fixed
second heart sound (96.2% vs43.37o),ejection
systolic
murmur
(IOO%vs
57.57o), anddiastolic flow
murmur
(26.4%
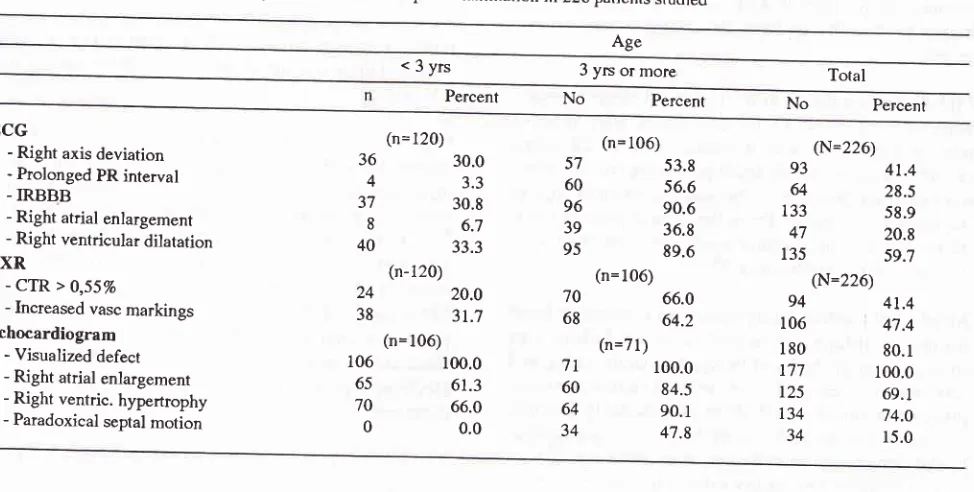
vsOTo),The results
of
supporting examinations
are presentedin
Table 5.
In this
table patients were also
arbitrarily
divided
into
2 groups,i.e.,
those aged 3 yearsor
more, and those aged lessthan 3
yearsold. Similar to
thoseof
the
clinical
findings,
we
also noted
that
typical
findings
for
ASD
were morecommonly found in older
patient
group when compared
with
those
in
younger
patients.
Notable difference
was noted
in
theprolon-gation
of
P-R interval
(56.67oin
group
of
patients
3years
of
ageor more
vs3.3%
in
those aged less than 3years), incomplete bundle branch
block
(90.67o
vs30.870),
right ventricular
hypertrophy (89.6%
vs33.37o).
Cardiothoracicratio
ofl more than
55%
and increasedvascular markings were
2times
asmuch
in
the
group
of
patients aged
3
years
or
more
asin
theyounger
agegroup.
With
echocardiograms, the atrial
septal defect
could be
seenin all
subjects examined
(106 patients
in
group
lessthan
3 yearsof
ageandTl
patients in the oldergroup). Right atrial
andventricular
dilatations
were also noted morefrequently
in theolder
age
group.
Of particular
interest was that
we did
notfind
aclear paradoxical septal
motion in
theM-mode
of patients
less than 3 yearsof
age, butdid
soin
32.1%of
patients
aged 3 yearsor
more.Age
$ears)
1983-1986 (without echo)1987-1992
(with echo) Total
<3
3 or more
t4 (28.670) 3s (71.4%)
tO6
(59.9Vo)
l2O (53.57o)'tr
(40.r%)
106 (46.5%)Total 4e (too%) r77 (roo%) 226 (rOO.O7o)
The clinical
symptoms and signs
of
the 226
patientswith ASD
2o areshown
in
Table
4.The patients
werearbitrarily divided into 2
groups, i.e.,
those aged lessthan
3
years and those aged
3
years
or
more.
The
division
was based on the assumption that at the age of 3 years theclinical
presentations ofASD,
if
any,usual-ly
havemanifested.
It
is seen that the percentageof
theclinical
manifestations
in
group
of
patients
aged
3years
or
more was consistently higher than that
of
Table 4. Physical hndings of the226 patients studied
Age
< 3 yrs (N=120) 3 years or more (N=106) Total (N=226)
Percent Percent Percent
Dyspnea on exertion
Recurrent respiratory tract infection Tachycardia
Growth retardation Right precordial bulging Right precordial heaving
Thrill
Pulmonary tapping
Accentuated first heart sound Widely fixed
split
2nd heart sound Accentuated P2Ejection systolic murmur
Mid diastolic tricuspid flow murmur
[image:3.595.56.549.488.734.2]Atrial Sepral
Defed
45 Vol 5, No 1, January -March
1996Table 5' Results of ECG, chest X-ray, and echocardiohraphic examination in 226 patients studied
Ag"
<3yrs
3 yrs or moreTotal
Percent No Percent No Percenl
ECG
- Right axis deviation - Prolonged PR interval
-IRBBB
- Right atrial enlargement
- Right ventricular dilatation
cxR
-
cTR
> 0,5570- Increased vasc markings Echocardiogram
- Visualized defect
- Right atrial enlargement
- Right ventric. hypertrophy
- Paradoxical septal motion
(n= 120)
36
30.04
3.337
30.88
6.740
33.3(n-120)
24
20.038
3t.7(n=106)
106 65 70 0
100.0 61.3
66.0 0.0
57 60
96
39 95
70 68
71
60 64 34
41.4 28.5 58.9 20.8 59.7
4t.4 47.4
80.
I
100.0
69.1 74.O
15.0
(n= 106) 53.8
56.6 90.6
36.8
89.6 (n=106)
66.0
64.2
(n=71)
100.0 84.5 90.1 47.8
(N=226)
93 64
133
47
135
(N=226)
94 106 180
t77
125
134
34
Cardiac catheterization Simple ASD closure Surgical mortality
We performed cardiac catheterization
in
36out
of the
total 226
patients.
Most
of
them
(27)
are performed
beforeechocardiography
was available,AftËr
echocar_diographic examination
wasavailable,
wedid cardiac
catheteronly in
patients who
showed evidenceof
pul_monary hypertension. Surgical closure
of
the ASD
was perfomed
in
47
patients,
with
the mortatity
of
8.5%.
SeeTable
6.Table 6. Invasive diagnostic procedure and snrgical cases
Hospital
in
Boston reflecting the recent
increase in
atrial
septal defects,probably
relatedto
local
interestsin closing
these defectswith
devicesintroduced during
cardiac catheterization.3 We
can saywith
confidence
tha
n the number
of
patientsdia
20
in the last
5
years
isclo
bility
of echocardiographic
examination.
Similarly,
the
incerased number
of
patients
aged less than 3 yearsin
our
series must havebeen
related
toechocardiography.
Our
dataalso support
previous
knowledge that ASD
patients aged less than
3 years
of age are
usually
asympetomatic,
and
alsogive only
non_specificclinical
signs."-
''
Typical auscultatory findings
ior
ASD which
areconsisted
of widely fixed
second heart sound andsoft
ejection
systolic
murmur are usually noted
whenthe
patients becoming
older,
sothat
prior
to
echocar_diography
era, thediagnosis
of ASD is
usually
estab_ lishedin
the preschool agegroup
(3_5 years). Thewide
split
of the
second heart sound
resulis front
delayedemptying of
rheoverload
right
ventricle;
thefixed
split
is
the
consequenceof
unlintited conrntunication
be_tween the
two atria, allowing
for
equalization
of
theinfluence
of
respiratory
variation
on
theright
andleft
ventricular
output.3Other non-specific
findings
in
ASD
include right
precordial bulging
andrighr precordial
heaving, Thèse arecorrelated
with right ventricular volume
overload
with
largeleft
toright
shunt atatrial
level. This
abnor_mality
is
usually found when the overload
become36 (ts.e%)
47 (2O.8Vo)
4
(
8.s%)DISCUSSION
problem constitute
onegroup,
whereasolder children
contribute to
the second peak.3The
inceras
morepatients
dia
period,
has
.ii:
[image:4.595.46.533.97.343.2] [image:4.595.38.552.100.334.2]46
Madiyono et al. Med J Indonesatrial
pathway
which
conducted faster
thansurround-ing atrial
muscle; and
(2)
the
right atrial
enlargementrequired
to
accommodate
the
hemodynamic volume
overload
increases the distanceofthe
SA node and theAV
node.7'loChest
x-ray in ASD
showed moderate to marked
car-diomegaly with
increasedpulmonary
vascular
mark-ings,
proportionate
to the amount of shunt.3'7'22 In mostca_se^s, the
pulmonary artery
segment wasprominent.l-rtt'zz
In
this
series,cardiothoracic
ratio of
greater than0,55
and increasedvascular
marking
were
seenin
94 cases(41.4%) and 106
cases(47.4%),
respectively.
When we
divided
the patientsinto
2 group wi th a cutoffpoint of
3 years (seeTable 5),
it
became apparent thatthose
abnormalities
weremainly
seen in older patients.Hoffman rqlorted
that large shunt
might
have nocar-diomegaly.e
The echocardiographic diagnosis
of ASD
hasevolved
to
thepoint
where
it
can be madewith virtual
certain-ty.r
Combined
normal findings
by
x-ray
film
andechocardiography
appeared adequatefor
exclusion
of
ASD.14
ASD
are best
visualized using a
subxiphoid
view. In this
series the defectcould
bevisualized in all
177 cases
(Table
5).Supporting evidence
for
a shunt should always
besought. Reversal septal
motion on the M-mode
asmanifestation
of
right ventricular dilatation could
bedetected
in
34 cases (15.O%of
all
cases).It
isinterest-ing
to note that nosingle patient
aged less than 3 yearsshowed reversal septal
motion.
Right atrial
enlarge-ment anddilatation of
theright
ventricle
thatindicated
volume loading
due to theleft-to-right
shunt wasfound
in
125
casesand
134
cases,respectively. Value
of
respiratory variations dimension
by echocardi ographi cstudy in
theidentification
of small ASD2
notrequiring
surgery had been
reported. 15A
normal
right
ventri-cular
end-diastolic dimension
during expiration
(RVDDE) is
very
specific
but not sensitive,
anormal
septal
motion
is
very
sensitive and
moderately
specific,
andnormal variation in
right
ventricular
dias-tolic with
respiration
(RVDVR)
is both very sensitive
and
specific.ls Doppler color
flow
mapping
is
espe-cially useful
in
detecting shunt
flow
acrossan atrial
defect.3
Transesophageal echocardiography has
overcome
some
of
the
limitations of
thetransthoracic
approach.Tiansesophageal
Doppler color flow
imaging
is
ex-tremely
sensitive notonly in detecting ASD
but alsoin
evaluaiing
the
size and the shunt
flow
volunr".16
chronic;
in
the
caseof
ASD, older children
have
thehigher probability
to
have this sign,
as seen
in
our
series.
Mid-diastolic
murmur
at thelower left
sternal border,
whis
is
considered
to
be
associated with
relative
tricuspid
stenosis was detected
only
in
28
cases(12.4%). This
relatively
small
percentageof
mid-dias-tolic murmur
wâs due
to
the
absenceof
such
sign
in
the younger age group.
From
theclinical
point of
view,
the presence ofthis murmur usually
indicates that there is alarge
left
toright
shunt.3i'7
Atrial
septal defect
rarely
results
in
congestive
heartfailure
in
infancy.
Congestive heart
failure
was
suspected
on the
basisof
tachypnea, tachycardia,
andcardiomegaly.
Early
changesin right
ventricular
com-pliance combined
with
ASD
can lead toearly
diastolic
overloading of
theright
ventricle
causingcardiomega-ly
andcongestive heart
failure
at
anearly age.'u
His-tory of
frequent respiratory
infections
wasreported
inmost
patients.lo We
did
not
diagnose
a single ASD
patient
with
frank congestive
heartfailure;
however,
asubstantial
number of
patients,especially
those aged 3yeils
or older,
showed growth
retâTdâtion.This
indi-cated
that
the
left to right
shunt
had
disturbed
thenormal
hemodynamic,
w-hich causedin
decreasedin-take
of
the nutrients.
17-20Patients
with
complicated
ASD
showed marked
retardation
in
both height
andweight;
whereas those
with
isolated
ASD
20 showedonly slight
retardation
in
height, but
moderateretarda-tion in weight./
Pulmonary hypertension
as a.consequenceof ASD
20develops
rarely in chilhood.''
Pulmonary tapping
and accentuated P2 as signs ofpulmonary
hypertension thatmay develop
in
untreated patients
were found
in l0
cases
(4.4%),
all of them
belonged
to the older
agegroup. These
findings
were confirmed
on
cardiac
catheterization.
Abnormal
electrocardiogram
areusually
seenin
ASD
2o.l-3 Ho*ever, this abnormality is
more commonly
seen
in older patients,
as also seenin
our series.In this
series
incomplete
right
bundle
branchblock
wasfound
in
133
cases
(58.9%) (Table
7). Incomplete right
bundle branch
block
was
mostly not
seenin
infants.
Right axis deviation
was
found
in
93
cases(41.1%).
Prolonged PR-interval
wasfound
in
64(28.5%).
Fyler
had also noted
prolonged PR-interval
in l0
per cent of,ASD
2() cases. There aretwo factors
thatcontribute
theprolongation
of the PR-interval:
(i)
any
large atrial
septal defect altered a large segment
of
the anatomyof
Vol 5, No 1, January - March 1996
fr-ilsnid
regurgitation
is adeterminant of
rheright to
left
shuntin
patients
with ASD
evenin
the absenceof
the
reversal
of
pressuregradient
betweenthe
left
andright atrium.'o
Cardiac catheterization
andsurgical closure
were per_formed in
36patients
(t5.9
%)
and 47 parients (20.8 %),respectively (Table
6).Most of
the cardiac catheteriza_,iol
*gl"ryrformed
before rhe adventof
echocardiog_laphy.t'zs'z+ The
pulmonary-systemic
flow ratio
> 2.5was
found in
most
casas, andhad
agood correlation
with
the presenceof mid
diastolic
tricuspid flow
mur_mur. Pulmonary vascular
resistance
was normal
in
most cases.
As
has beenpracticed
in
most centers, thesurgical
closure wasperformed in last
II
caseswithout
cardiac catheterization.
To
day the risk
of
cardiac
surgery
for ASD
20is
virtually
zero,but unfortunately
!!"_1*gt"ul
mortality
rate
in
this
series wasstill
higir
(8.5%) (Table 8). Four patients died,
consisredof
onepatient died on table
of
profuse bleeding and the
3others
deceasedless
than 24 hours afteisurgery
of
respiratory
and congestive heartfailure.
In view of high
rateof
spontaneousclosure
evenof
a largeASD, it
seems advisable to defer electivesurgical
closure
until
after 2-3
yearsof
ageif
successful medi_cal
rnanagement can be ac tieved.3'8Most infants
with
symptomatic
ASD
may
be managedmedically,
allow_ing
sufficient time to
observe
*h.th",
spontaneousclosure
will
occur. 12Vigorous
medical
mànagement,including
digitalis,
diuretics,
andantibiotics,
were suf_ficient
tomaintain
theseinfants during
thiscritical first
year permitting elective surgical repair
later.l0
In
symptomatic infants who
fail
to
respond
to intensive
medical therapy
thedefect is
best clôsedimmediately,
both
to improve
the
clinical condition
andto
preventthe
development
of
further
pulmonary
vascular
damf8-e.
Though pulmonary hypertension
developsrarely in childhood,
closureof
the defect should not be postponedif
there is any doubt thatpulnronary arterial
is
normal.2l Double-umbrella
devices that areinserted
with a
cardiac catheter are
now
used
to
close many
ASDs.
The
desirability
of avoiding
intrathoracic
dis_section
andopening
the hearti,
"Uiio*.i-'-SUMMARY
3.
swith ASD
20 rheclinical findings
ot specific,
echocardiographic
ex_usually
needed toconfirm
the diag_ nosis.4.
Growth retardation, cardiomegaly,
right
bundle
branch
block,
right
ventriculai
hypertrophy,
paradoxical ventricular
septal
motion,
were
com_ monin
largeASD
20.5.
Simple closure of
ASD
2o
was the
procedure
of
choice.
REFERENCES
l. Feld
RH, Edwards WD, puga FI, Seward JB, Weilman WH.Atrial septal defects and atrioventriculap canal, In: Adams FH, Emmanouilides GC, eds. Moss. Heart disease
in
in_fants, children and adolescent; 3rd ed. Baltimore: Williarns
and Wilkins, 1983; 1lB-34.
2. Berman LB, Zuberbuhler JR. Atrial septal defect. In: Ander_
son
RH,
ShinebournEA,
Macartney FJ, TynanM,
eds.Pediatric
Cardiology,
lst
ed. New
yoÀ:
Churchill
Livingstone, l9B7
;
541-62.:.
fflgr
DC. Nadas' pediarric cardiology. Singapore: Hanley Belfus, 1992;513-24.4. PerloffJK. The clinjcal recognition ofcongenital heart dis_ ease; 3rd ed. Philadelphia: Saunders, l9g7 ; 27 2_349 5. Baum D, Beck R, Kodama A, Brown B. Early heart failure
as cause
of
growth and tissue disorderin
children with congenital heart disease. Circulation 1990; 62:1145_51.6. Sastroasmoro S, Oesman IN, Macliyono B. Auskultasi jan_
tung dan fonokardiografi, Naskah Lengkap pendidikan Tambahan Berkala Ilmu liesehatan AnaÈke-XI. hal. 5_20
(Fakultas Kedokteran Universitas Indonesia, Jakarta l9g5). 7. Madiyono
B,
OesmanIN,
Sastroasmoro S, Sukman Tp, Soelaiman EI, Rachmad KB. Secundurn atrial septal defect-
lfore
and aftersurgery. pediatrlndones l9g9;29 :, 199_20g. 8. Hunt CE, Lucas RV Jr. Symptomatic atrial septal defect ininfancy. Circulation 197 2; 47 : l}42_g.
9. Hoffman JIE, Rudolph
AM,
DanilowiczD.
Leftto
right atrial shunt in infants. Am J Cardiol 1972;3}:g6g_75. 10. DimichI,
Sreinfeld L, park SC. Symptomaric atrial septaldefect in infants. Am Heart
I
1973; g5:601_4.I l. Tandon R, Edward JE. Atrial septal defect in infancy. Com_
mon association
with
other anomalies. Circulation 1974; 49:1005-10.12. Mahoney
LT,
Truesdell SC, Krzmarzick TR,huer
RM.Atrial septal defects that present in infancy. Am J Dis Child
1986; 140: l l l5-8.
13. Madiyono
B,
OesmanIN,
Sastroasmoro S. pemeriksaan ekokardiografi pada beberapa penyakit jantung bawaan.Naskah Lengkap pendidikan Tambahan Berkala Ilmu Kesehatan Anak ke-XI, hal. 43_70 (Fakultas Kedokteran Universitas Indonesia, Iakarra l9g5)
14. Egelblad H, Heming J, Efsen F, Wennevold A. Non_invasive
diagnosis in clinically suspected atrial septal defect ofsecun_ dum or sinus venosus type. Value ofcombining chest x_ray,
ptronocardiography, and M-mode echocardtgarphy. Ér Heart
f
980;44:lt7-21.
Atrial Septal Defect
The
data:
following
features can be summarized
from
our
1. ASD
20affected
girls
more than boys, the sexratio
was
1.5:1.2.
Typical auscultatory findings could be heard in
48
Madiyono et aI.15. Mauran
P,
Fouron JC, CarcellerAM,
et
al.
Valueof
respiratory variations of right ventricular dimension in the
identification of small atrial septal defects (secundum type)
not
requiring surgery:An
echocardiographic study. AmHeart J 1986; 112:548-53.
16. Kai H, Koyanagi S, Hirooka
Y,
etal.
Right{o-left shuntacross atrial septal defect related to tricuspid regurgitation:
Assessment by transesophageal Doppler echocardiogarphy. Am Heart
I
1994;127:578-84.17. Mehrizi A, Drash A. Growth disturbance in congenital heart disease. J Pediatr 1962;67: 418-29.
18. Feidt RH, Stricler GB, Wiedman WH. Growth of children
with congenital heart disease. Am J Dis Child 1969;
ll7:.
573-9.
19. Suoninen P. Physical growth
of
childrenwith
congenitalheart disease, pre and post operative study of355 cases. Acta Paediatr Scand 1971; Suppl 255:1-45.
20. Chan KY, Tay JSH, Yip WCL, Wong HB. Growth
retarda-tion
in
children with congenital heart disease. J SingaporePaediatr Soc 1987; 29:185-193.
Med J lrtdones
21. Haworth SG. Pulmonary vascular disease in secundum atrial
septal defect in childhood. Am J Cardiol 1982;5I:265-12, 22.'lamaela LA. Penilaian X-foto polos pada penyakit jantung
bawaan, Naskah I-engkap Pendidikan Tambahan Berkala Ilmu Kesehatan Anak ke XI, hal. 5-20 (Fakultas Kedokteran Universitas Indonesia, Jakarta 1985).
23. Madiyono
B,
TrisnohadiHB, Affandi
MB.
His
bundleelectrocardiogram
in
children with secundum atrial septaldefect. Paediatr Indones 1981; 21:1-10.
24. Oesman IN, Madiyono B, Sastroasmoro S. Kateterisasi jan-tung dan angiokardiografi pada penyakit jânjan-tung bawaan,
Naskah Lengkap Pendidikan Tambahan Berkala Ilmu
Kesehatan Anak ke
XI,
hal. 71-84 (Fakultas Kedokteran Universitas Indonesia, Jakarta I 985).25. Rachmad KB. Tindakan pembedahanjantung pada penyakit jantung bawaan; Naskah tengkap Pendidikan Tambahan Berkala Ilmu Kesehatan Anak ke
XI,
Hal. 88-96 (Fakultas Kedokteran Uni versitas Indonesia, Iakarta 1 985 )26. Graham TD. When to operate on a child with congenital