5
Artawan Eka Putra et ol. &MC HeoM Seruices Rueorch 201 3, 13:445
http://www.biomed central.com/1 47 2-6963 / 1 3 I 445
(n
Health
Services ResearchFactors
associated
to
referral
of
tuberculosis
suspects
by
private
practitioners
to
community
health
centres
in
Bali Province, lndonesia
I Wayan Gede Artawan Eka Putra1", Ni Wayan Arya Utamil, I Ketut Suarjanar, I Made Kerta Duanal,
Cok lstri Darma Astiti2, lW Putra3, Ari Probandaria, Edine W Tiemersmas and Chatarina Umbul Wahyuni6
Abstract
Background: The contrast between the low proportion of tuberculosis (TB) suspects referred from private practitioners in Bali province and the high volume of TB suspects seeking care at private praclices suggests problems with TB suspect refenal from private practitioners to the public health sector. We aimed
to
identifu key factors associated with the referral of TB suspects by private practitioners.Methods: We conducted a case-control study conducted in Bali province, lndonesia. The cases were private practitioners who had referred at least one TB suspect to a community health centre between
I
January 2007 andthe start of data collection, while the controls were private practitioners who had not referred a single TB suspect in
the same time.
Results: The following factors were independently associated with referral of TB suspects by private practitioners: having received information about the directly observed treatment short-course (DOTS) strategy (OR 2.0; 950/o Cl 1.1
-38), ever having been visited by a district TB program officer (OR 2.1; 95o/o Cl i .0-
4.5), availability of TB suspect referralforms in the practice (OR 2.8; 95Vo Cl 1.5-5.2), and less than 5 km distance between the private practice and the
laboratory for smear examination (OR 2.2; 95Vo Cl 1.24.0).
Conclusions: Education and exposure of private practitioners to the TB program improves referral of TB suspects from private practitioners to the national TB program. We recommend that the TB program provides all private practitioners
with information about the DOTS strategy and TB suspect referral forms, and organizes regular visits to private practitioners.
Keywords: Tuberculosis, Private practitioners, Operational research, lndonesia
Background
Indonesia has a high burden
of
tuberculosis (TB) withapproximately 450,000 new patients
in
2010 [1].Multi-drug
resistant (IvIpR)TB, which
is
more difficult
totreat, may q{nerge
if
TB is not appropriately treated and has been associatedwith
the presenceof
an importantprivate sector [2]. Private practitioners often do not
fol-low the directly observed therapy, short course (DOTS)
strategy [3]. Several studies showed that poor adherence
to
the DOTS strategy leads to poor treatment outcomes* Conespondence [email protected] 1- ,
'Schooi oi Pubiic Health, Faculty of Medicine, Udayana Uriversiry, 6ali, lndonesia
Full list of author information is available at the end of the article
[a]. To increase the coverage of DOTS treatment, the
in-volvement
of
private practitionersin
aTB
control pro-gram is essential [5,6].Although the absolute contribution to TB case finding
and treatment is not exactly known
for
most countries, some studies from different Asian countries suggest thatprivate practitioners may play an important role
in
thediagnosis and treatment of
TB
[6,7].In
Indonesia, ana-tional
surveyon
health seeking behaviour among TBsuspects
in
2004 showed that 54% first sought treatmentwith
private practitioners[8].
A
study involving tele-phone interviewsof
25%of
the private practitioners in|ogjakarta province showed
that most private practi
tioners (63%) reported to have seen TB suspects in their
f \
@ 2013 Artawan Eka Putra et al.; licensee BioMed Central Ltd. This is an open access article dlstributed under the terms ofthe(
J
Blotned
central
5ffffi,5;:tr[#J'};ri1i,h':ffimJl,T:31["sffiT.'J?l3i'f:l-",1i,'Ji?i;H:$ *rmi"
J
Artawan Eka Putra et ol, BMC Heolth Services Research 2013, 13:i{45
http://www.biomedcentral.com/l 47 2-6963 I 1 3 I 445
private practice. Almost one-third of the interviewed
pri-vate practitioners neyer referred a TB suspect to the
na-tional
TB
control program (NTP)
for
diagnosis andtreatment and
most
of
these private practitioners didnot offer DOTS treatment [9].
A
studyin
Bali reportedthree main problems associated with TB care within the
private sector: poor TB treatment adherence among
pa-tients, limited
capacityof
public
servicesand
poor public-private integration [10].Since 2004, a partnership program
in
BaIi has encour-aged 537 private practitioners (23 specialists, 151 medicaldoctors, 189 midwives, and 154 nurses)
to
participate inthe
TB
conffol program. However, only 2.8%of
TBsus-pects identified
by the
TB
control
program had been referred to a community health centre by a private practi-tioner [11]. This finding contrasts with the high volumeof
TB suspects seeking care at private practices as found in
the above-mentioned studies and suggests problems with
TB suspect referral from private practitioners to the public health sector. We aimed
to
identify factors associated toreferal
of
TB
suspectsby
private practitionersin
Bali, Indonesia.Methods
Design
We performed a case-control study.
A
case was defined as a private practitioner who had referred a TB suspectbetween
I
)anuary 2007 and the start of data collection.A
control was deffned as a private practitioner who hadnot referred any TB su$pect to the public sector over the same time period.
Study settings
The study was conducted
in
Tabanan and Karangasemdistricts
in
Bali province, Indonesia. Tebanan is locatedin
West Bali and Karangasemin
East Bali. Thesedis-tricts
were selected because they are representative forwhole
of
Bali
in
many respects.\fhile
many privatepracfitioners serve in both areas, a relatively low
propor-tion of all TB
suspects registeredin
community healthcentres
in
TabanaR;district had been referredby
apri-vate practitiimer (f.1%) in2OO7, whereas this proportion
was relatively
high
for
Karangasem (L{.L%), Tabananand Karangasem are
rural
districts.In
2007, Tabanan and Karangasem were inhabited by 4A7,L62 (485 persons/ km2) and 982,939 persons (456 persons/km2), respectively.In
20f7,
there were61
physicians and 324 midwives/ nurses (paramedical staff examining and keating patients especiallyin
remote areas)in
Tabanan andN
physiciansand?M midwives/nurses in Karangasem [12,13].
Study population, sample size and sampllng design
The study population consisted
of
private practitionersin
Bali
Provinceincluding
pulmonologist, internists,Page 2 of 6
general practitioners, midwives
and
nurses. W'e used Kelsey'sformula
[14]for
sample size calculations, and assumed that the proportion of private practitioners ex-posed to information about the DOTS program was 25%among cases (P1) and 10% among controls (Pd. We cal-culated that a minimum sample size of 92
in
each groupwas neede4 taking a ratio
of
casesto
controlsof
1:1, asignificance level
of
5% and a study powerof
80%. We aimedto
include 100 persons per groupto
accountfor
losses due to partial participation.
The
study used multistage cluster randomizedsam-pling. First, Tabanan and Karangasem district were
se-lected purposively
from nine
districtsin
BalL becausethe two districts represented the extremes
in
thecontri-bution of private practitioners
to
the referral of TBsus-pects
to
communityhealth
centres (see above). Werandomly selected 10 community health centres
in
eachdistrict.
Then,we
randomly selectedl0
private practi-tionersin
the coverage area of eachofthe
selected com-munity health centres from a list that contained all private practitioners in the two districts bytpe
of practitioner.Data collection and analysis
Data were collected by interviewers using pre-structured guestionnaires
that
had been piloted among 15 private practitioners duringa
smallpilot
studyin
anotherdis-trict
(Gianyar).We
collectedinformation about
thecharacteristics
of
the private practitioners (gendeX, age,occupation, and qualification), work experience, opening
hours per day, availability
of TB
suspect referral formsin
the private practice, and distance of the participant'sprivate
clinic
to
a
sputum smear laboratory. Also, weasked whether the respondent had ever received
infor-mation about
DOTS, whetheror
not
the
participant could rememberto
have been visited at least once by aTB officer (the officer who is responsible for the conduct of the TB program
in
districts). We assessed the respon-dent's knowledge about the DOTS $trategy by asking 11multiple-choice questions. The questions covered three basic competencies that medical doctors should have in
relation to TB ease management, i.e. TB suspect
identifi-cation, diagnosis and
treatment The
11 questionscov-ered signs and symptoms
of
adult
and childhood TB,laboratory diagnosis, diagnosis
of TB in
children,num-ber
of
sputum samplesto
be analysedfor
diagnosisof
TB, type of sputum examination for diagnosis, timing
of
the start
of TB
keatment, antiTB
drugs, costof
treat-ment, duration of treatment and the importance
of
dir-ect observation. Good knowledge was defined as having answered more than
5 of
these 11 questions correctly,while having less than five correct answers was
catego-rized as poor knowledge.
We kained four interyiewers
to
perform the dataj
Artawan Eka Putra et al, BMC Heolth Sevices Reseorch 201 3, 13:445
http://www.biomedcentra Lcom/l 47 24963 / 1 3 / 445
private practitioners.
If
they agreedto
participate, anap-pointment
for
interview was made. The privatepracti-tioners were interviewed in their office by the study team.
Of
200 private practitioners who had been invited toparticipate
to
the
study,all
agreedto
be
interviewed.However, only 181 (9O,5%;94.O% of the cases and87,O%
of the controls) were present at the appointed date and
time
of
the
interview.The
private practitioners whocould
not
be
interviewedwere more often
specialist(pulmonologist and internist) than those who were inter-viewed.
A
private practitioner who r,rasnot
available atthe time of interview was replaced by the private
practi-tioner appearing above the selected private practitioner
on the list.
If
this private practitioner wasnot
availableat
the time
of
the
interview,the practitioner
belowthe initially
selectedpractitioner
was chosen instead,so
that the total
study population included 100 casesand 100 controls.
'We used Chi square tests to
identiff
univariateassoci-ations between private practitioner characteristics and
TB suspect referral. Backward logistic regression models
included ali variables with a p value < 0.25 in the
univari-ate analysis (Chi square test).
The
ethical clearance was obtainedfrom the
EthicsCommittee of the Faculty of Medicine, Udayana Univer-sity and the permission
to
implement thettudy
wasob-tained
from the
NationalUnity
and Public ProtectionBody (Kesbanglinmas), Bali Province.
Results
Of
a totalof
200 private practitioners, 100 practitionerswho had referred at least one TB suspect to the TB
con-trol
program (cases) between1
fanuary 2007 and thestart
of
data collection and 100 practitionerswho
hadnot done this (controls) were included
in
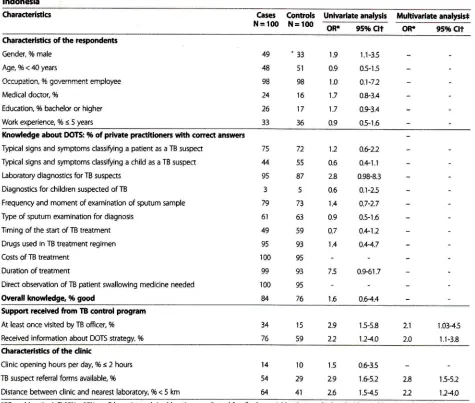
the study. Thegeneral characteristics
of
the
casesand controls
aregiven in the able.
In
comparisonto
controls, cases weremore often
of
male (49% vs 33%). Also, the proportionof physicians was higher among cases than among
con-trols
(24%vs
16%),but
thls difference wasnot
statisti-cally significant. Tiiere were no differenceswith
respectto the othercharacteristics listed in the table.
Most
respondents (96%) lacked knowledge about the diagnosis of TBin
children and only part of them (49%)was able
to
correctly indicate whenTB
therapy shouldbe
started,Almost
all
respondents correctly answeredthe other
knowledge questions, suchas the
needof
appointing
a
treatment observer,the duration
of
TBtreatment and the anti-TB dprgs that constitute a
stand-ard
TB
regimen. There wasno
signiffcant difference inoverall knowledge between private practitioners who
re-ferred TB suspects and those who did not refer TB
sus-pects
to
the
healthcentre (OR
1.6; 95% confidenceinterval (Cl) 0.6-4.4).
Page 3 of 6
Among the
practitionerswho
reportedto
havere-quested sputum smear examination from a laboratory at least once
in
the past year (N = 100), 28% reported that they had never received the resultsof
the examination.Private practitioners
who
had referredTB
suspects topublic healttr" centres were more likely
to
have receivedinformation about
the
DOTS strategy (OR 2.2t 95% CI1.1-3.5), been visited
at
least once by aTB
officer (OR 2,9t 95%CI
1.5-5.8), have TB suspect referral forms avail-able (OR 2.9;95%CI
1.6-5.2) and havetheir clinic
at adistance of less than 5 km from a sputum smear
labora-tory
(OR 2.6t 95%CI
1.5-4.5). The multivariate analysis showed that all these factors were independently associ-atedwith
referring TB suspectsto
a public health facility(Table 1).
Discussion
The results of this study reveal that the provision of
in-formation about
the
DOTS strategy and referralof
TBsuspects are important
to
improvethe
referralof
TBsuspects by private practitioners to public health centres. Private practitioners who had referred TB suspects were
more likely to have been visited by a TB officer, have
re-ceived
information
aboutthe DOTS
strategy,and
tohave referral forms available than the practitioners who had not referred a single TB suspect A TB office.r, when
visiting
a
private practitioner,is
expectedto
remind practitioners about their rolein
ffnding TB suspects andabout the importance
of
sendingTB
suspectsto
public health facilities for microscopic waluation.A
studyin
Myanmar concludes that the successfac-tors of the private practitioners'contribution to TB
con-trol
were training and supervision bythe
public sectorand provision
of
drugs and consumables freeof
chargeby the NTP
[15].A
study aboutthe
processof
col-laboration between
NTP and
hospitalsin
Yogyakarta,Indonesia, reveals that partnership can be established
if
it
beginswith
an intensive process of interactioninclud-ing
intermediary actors (i.e., persons approaching theprivate hospital and advocating the partnership program)
for
approachingthe NTP
andthe
hospital [16]. Other studiesfrom
different countries and on differentconti-nents show that the success
of
public-privatemix
pro-jects largely depends on the level of interaction between
private and public health care providers [17,18].
Our
study also indicated important enablersof
refer-rat
the availabilityof
officialTB
suspect referral forms and of a smear examination laboratorywithin
thevicin-ity
of
the
privateclinic.
Private practitioner's patientswho
had been referredto
a public
facility were morelikely
to
have visited a microbiology laboratory locatedwithin 5 km
distanceof
the private clinic. The balancebetween
the
benefitof
receivinga
laboratory&
Artawan Eka Putra et al, 9MC Heolth Serukes Rexorch 2013, 13:445
http//www.biom edcentral.com/1 47 2-6963 I 1 3 / M5
Page 4 of 6
Table
t
Factor associated to re{erral of TB suspectr to communlty hcahh centrus by pilvatc practitlonerc ln Bali provincc, lndonerlaCharacteristlcs
Gres
ControlsN=1&)
N=l(X!Unlvarlateanalysls Muhivadateanalyrls*
oR.
95%Ctt OR!
95% Ctt Characteylstlcs of the respondemsGender, % male
Age,%<40years
Occupation, % government employee
Medical doctor, (t6
Education, % bachelor or higher
Work experience, % < 5 years
49
48
98 24 26 33
'33
51
98 16 17 36
1.9
1.1-3.50.9
0.5-1.51.0
a.1-7.21.7
0.8-331.7
0.9340.9
0.5-16Knowledge about IXITS: % of prlvate pmctitloneE wlth conect amwers
Typical signs and symptoms classlfuing a patient as a TB suspect Typical signs and symptoms dassif,ing a child as a TB suspect Laboratory diagnostics for TB suqqects
Diagnostics for children suspected ofTB
Frequency and moment of examination sf sputum sample Type of sputum examination for diagnosis
Tlming of the start of TB treatment
Drugs used in TB treatment regimen
Costs of TB treatment Duration of treatment
Direct observation of TB patlent swallowing medicine needed
Overall knowledge, 96 good
7q 44 95 3 79
61
49
95 100
99 100
u
72 55 87 5 73 63 59 93 95 93 95 76
1.2
4.G2.20.6
0.+1.12.8
0.98€.30.6
0.r-2.51.4
0.7-2.70.9
0.5-1.60.7
0.+1.21.4
0.+4.77.5
4.941.7r.6
a.ilA
Suppo* received ftom IB control prognm At least once visited by TB officec % Received information about DOTS strategy, %
34 76
15 59
2.9 2.2
2.1
20
1.5-5.8 1.24.0
r.03-4.5 1.1-38
Chsrad€ristlcs of the dlnk
Clinic opening hours per day, % < 2 hours TB suspect referral forms available, %
Distance between clinic and nearest laboratory, % < 5 km
2.8 2.2 14
54
&
'10
29 41
1.5
0.63.52.9
1.&-5.22.6
r.54.51.5-5.2
124.0
*OR
= odds ratio; t O 95% = 959t conftdence interval; * odds ratios a.e adjust€d for all other variables that are displayed with an odds ratio in thi5 table.
laboratory is more likely to be rated positive by TB sus-pects
if
they have a laboratory for sputum smear nearby. Private practitioneis having refemal forms available weretwice mord-likely
to
refer suspects than those who didnot have such
foms.
Referral slips were successfullyin-troduced
in
private practicesearlier
[19],but
to
ourknowledge, this is the fust study indicating that the pres-ence of referral forms alone is an important enabler for
referral of TB suspects from private practitioners
to
thepublic sector.
An
important factor that may discourage privateprac-titioners
to
referTB
suspectsis the
lackof
feedbackfrom the
community health centre aboutthe
sputum examination result of theTB
suspect that they referred.Almost
onethird of
private practitionerswho
hadre-ferred
TB
suspect(s)to a
sputum
smear laboratorydeclared that they had never received the sputum smear
result of these suspects. Private practitioners not
receiv-ing any feedback on the test results of
TB
suspects canbe expected
to
get discouragedin
referring suspectbe-cause they
feel not
appreciatedfor
their
participation and they also may get the impression of losing patients because these do not go back to private practitioners.In-deed, when private practitioners were asked about their
wishes
with
respect to public-private collaboration, mostof
them indicated that they desiredto
receive adequateand timely feedback
of
the public health facilities (datanot shown).
Our
study had some limitations. Finst,we
includedonly part
of
the private practitionersfrom two
districts [image:4.600.64.539.107.510.2]t
Artawan Eka Putra et at. BMC Heolth Seruices Research 201 3, 13:2145
http//www.biomedcentral.com/l 47 2-6963 / 1 3 / 445
private
practitionerswere
randomly selected,r{e
areconvinced that this study gives a good representation
of
private practitioner's characteristics related
to
referralpractices
in
Bali.
Secondwe
selected privatepracti-tioners as controls
if
they had not referred a TB suspectfrom |anuary 2007
until
the start of data collection, andas cases
if
they had done this. The probabilityof
refer-ring
aTB
suspectto the
public health sector may notonly depend on the private practitioner's characteristics,
but
alsoon the
clinic's patient load. Practitioners whosee more potential TB suspects per day may have more
experience
in
identiffing
$ymptomsof
pulmonary TBand are more likely to refer pulmonary TB suspects than private practitioners who rarely see patients with
respira-tory symptoms. Out of efficiency considerations, the
lar-ger practices may have received more attention from the
TB officer
in
the past than smaller clinics. However,as-suming that the opening hours per day can be regarded
as a proxy for the clinic's patient load, we found no
indi-cations
for
such an effect, as the proportionof
privatepractices
with
opening hours of>2
hoursper
day didnot
differ between the cases and controls (86%at
caseand 90% at control group, p > 0.05),
This study provides important information
to
the TBcontrol program about what factors enable the referral
of
TB
suspects by private practitionersto
public health care providers. The major benefit of the study is indirect, however.The
provincial health office was closely en-gagedin
this study fromits
start. The resultsfrom
thisstudy have generated a sense of urgency to engaging
pri-vate practitioners
in
TB case findingin
Bali. As anindir-ect
outcomeof
this
study,an
intervention
is
beingprepared
to
improve the engagementof
private practi-tionersin
Bali province. The intervention is aninnova-tive program
of
awarding participationcredit
points(PCP)
to
private practitioners that referTB
suspects topublic health facilities
in
order to improve their collabor-ationto
the existing public-private mix projects. Theef-fect
of
this
interventionon TB
casefinding
will
be closely monitored,, and,if
positive, the interventionwill
be expanded to other Indonesian provinces.
Conclusions
To
improveprivate
practitioners' involvementin
TBcase ffnding, district TB officers should invest in visiting private clinics
to
educate private practitioners about theDOTS program, and to provide referral forms of TB
sus-pect.
Also, bringing
laboratory services closerto
theclinic, e.g. by implementing a sample transportation
sys-tem,
may enableTB
casefinding
in
Bali.All
privatepractitioners
should
receive continuous
supportivesupervision and should be provided with high quality
in-formation about the DOTS program and referral forms
for
TB
suspects.Most importanth
this
operationalPage 5 of 6
study has provoked new interventions by the provincial
TB
office
to
increase participationof
private
practi-tioners in the diagnosis of TBin
Bali province.Competlng lnterertr
The authors declare that we have no competing interests.
Authors' contrlbutlons
IWGAEP designed the study, developed the data collecion toolS conducted
the interviews, data analysis and drafted the manuscrlpt. UNWA contribured
to the design ofthe study, developed the methodology, and helped designing the data collection tools. IKS contributed to designing the study, development ofthe methodology and collected the data. IWP provided background information about the TB program in Bali province and helped in designing the data collection tools. CIDA contributed to development of the data collection tools, provided'lB related epidemiological information and helped with data collection. IMKD contributed to data collection and drafting of the manuscript. AP, EWT and CUW critically reviewed all aspects of the study and assisted in writing the manuscript. All of the authors have approved the final manuscript.
AcknotdcdgemenB
This research was funded by a grant from TBCARE-I of USAID- Also, the authors would like to thank TBCARE-1 of USAID for facilitation of a report and manuscript writing course in which the first author pafticipated. Furthermore, the authors are grateful to the Ministry of Health of the Republic of lndonesia and the Tuberculosis Operational Research Group of
lndonesia for thek suppon. The authors would like to thank all respondents
who kindly conxnted to participate in this study. We sincerely thankTB officers in Tabanan and Karangasem for their support and provision ofTB
related epidemiological information,
Funding
This study was funded by a grant from TBCARE-I of USAID.
Author detalls
'School of Public Health, Faculty of Medicine, Udayana University. Bali,
lndonesia. ?iIIP of Bali Province Health ffice 8alt, lncionesia. ilirT of
Tabanan District, Health Office, Bali, lndonesia. aDepartment of Public Health, Faculty of Medicine, Universitas Sebelas Maret, Surakana, lndonesia. 5KNCV Tuberculosis Foundation, The Hagug The Netherlands.6Faculty of Public Health, Airlangga Unlverslty, Surabaya, lndonesia.
Received: 17 April 2013 Accepted:24 October 2Ol3 Published: 28 October 20I3
Refercnces
1,
World Health Organization: WHO repo* Globdl tuberculuis conttol: Theburden ol disease caused by TB. Geneva: WHO Press; 201 1.
2.
Caminero JA: MultidruE-reslstant tubcrculosls: epldemiology. risk factors and case finding. lnt J Tuberc Lung Dis 201 0 14{4)1382-390.3.
Quy Hl Lonnroth K Lan Nl Buu TN: Treatment results among tuberculosis patients treated by private lung specialists involved in apubllcarivate mix .project in Vletnam. lnt -/ Tub*c Lung Dis 20A3, 7(12):1139-1 146.
4.
Uplekar M, Pathania V Raviglione M: Private practitioners and public health: weak links in tuberculosis control. loncet 2001,358(9285):912-916.5.
Rangan SG, Juvekar 5K Rasalpurkar SB, Morankar 5N, Joshi AN, Porter JDH:Tuberculosis control In rural lndia: lessons from public-private collaboration. lnt J Tuberc Lutg Dis 2004,8(5)512-559.
6.
Uplekar M, Juvenkar S, Moranlor S, Rangan 5, Nunn P: Tuberculosis patient and practitioners in private clinic in lndla. lnt J Tuberc Lung As 1998,2Q4l:324-329.
7.
L6nnroth ( Thuong LM, Linh PD, Diwan VK Utilization of private and public health<are providers for tuberculosis symptoms in Ho Chi Minh City, Vietnam. ikf]lth Miq Plann ng 2001, ,16(l):47-54"8.
fulinistry of Health Republic of lndonesia: Report ofTuberculosis PtudlenceSuruey of lndonesio 2004. )akafta: Ministry of Health Republic of lndonesia;
10.
I
Artawan Eka Putra et al, BMC Heafth Services Resqrch 2013, t 3:445
http//www.biomedcentral.com/I 47 24953 I 1 3 I 445
Mahendradhau Y, Utarini A" Lazuardi U, Boelaen M, Stuyft PV: Pilvate praclitioners and tuberadosis case detection in Jogjakarta, lndonesia:
actr.ral role and potential. Trop Med lnt Heolth 2007, l2(10):1218-1224. Armini LPS, Utarini A, Mahendradhata Y: Ihe impact of Eivate
practitioners partnership to the dday of management and tlnancing of
tubeiculosis patient in Denpasar. lndanesion ) lkohh SeNice Monage 2W7, I0(M):166-172.
Health Office of Bali Province: Health proffle of Bali province 2007. Denpaw:
Health Office of Bali Province; 2@8.
Health and Family Planning Office of Tabanan Ai:trtict: lleahh ptofile of
Tabonan district 2007. Tabanan: Health and Family Planning Office of
Tabanan District 2008.
Health ffice of Karangasem Distrior:. Health ptofile of Karangasem distrid
2ffi7 Amlaqra:Health Office of Karangas€m Distric! 2008. lGlsey JL, Whittemore AS, Evans A5, Thompson Vfr: Mahods in AbseNational Epidemrblogy, New York Oxford Univenity Press; 1996.
Probandari 4 Utadni A, Lindholm L, Hu(ig A Life of a partnership: the
process of collaboraUon between the National Tuberculosis Program and the hospitals in Yogyakarta, lndonesia. Soc Sci Med 201 1,
73(9):1 386-1 394.
Chakaya J, Uplekar M, Mansoer J, et d/: Publicfrivate mix for control of
tuberculosis and TB*llV in Nairobi. Kenp: outcomes, opponunities and obstacles. lnt I luberc Lung As zffi,12(1ll:127+1278.
Malmborg R, Mann G, Squke SB: Systematlc assgsment of fte concept and pracdce of publlcfrivate mix for tuberculosls care and control. lnt J
Equiry Heahh 201 I, l0:49.
Maung M, Kluge H, Aye
I
et ol fuivate GPs contribute to lB control in Myanmar: evaluation of a PPM initiatfue in Mandalay Division. lnt J TubercLung Dis 20Cf,, I Q9):982-987.
Lonnroth K Karlsson M, Lan NTN, Buu TN, Dieu TIN: Refenlng TB suspectg
fiom private pharmacies to the Natlonal Tuberculosls Programme: experiences ftom two districts in Ho Chi Mlnh City, Vietnam. lnt J Tuberc
Lung Us 2(N3, 7( l 2): l 147-1 1 53.
dol:l 0.1 1 86 / 1 47 24963- I 3-+45
Clte Orls artlcle ar: Aftawan Eka Putra et al: Fadors associated to refenal of tuberculosls suspecb by prlvate practitionen to communlty health centres ln Bali Province, lndonesia. BMC Heohh krvices Research
2013 13:445.
Page 6 of 6
Submit your next manus$ipt to BioMed Central
and take
full
advantageof
. Convenient online submission
o Thorough peer review
. No spa(e (onstraints or color figure charges
o lmmediate publication on a(ceptahce
r lnclusion in PuhMrd, CAS, S(opus and Google Stholar o Research which is freely available for redistribution Il.
12.
13,
14.
15.
t0.
18.
Submit your manuscript at