JENIS ARTIKEL ILMIAH
dr. Rahayu lubis, MKes
MENGAPA PUBLIKASI ILMIAH PENTING
• Syarat kelulusan mahasiswa S1, S2 dan S3
• Merupakan kewajiban desiminasi hasil temuan ilmiah ke publik (oleh peneliti)
• Sarana menyampaikan ide dan pikiran pada publik (Media komunikasi ilmiah)
• Amanat Tridharma Perguruan Tinggi:
- Penyebarluasan Iptek
3
PENTING KARENA....
PROSES PENULISAN
ARTIKEL ILMIAH
SAAT PENULISAN
DRAFT TULISAN ANATOMI
PASCA PENULISAN
PENYUNTINGAN PUBLIKASI
PRA PENULISAN
BAHAN TULISAN KERANGKA TULISAN
PROSES PENULISAN
PERSIAPAN
PRA PENULISAN
PRINSIP KARYA TULIS TEPAT
JELAS
SINGKAT
SAAT PENULISAN
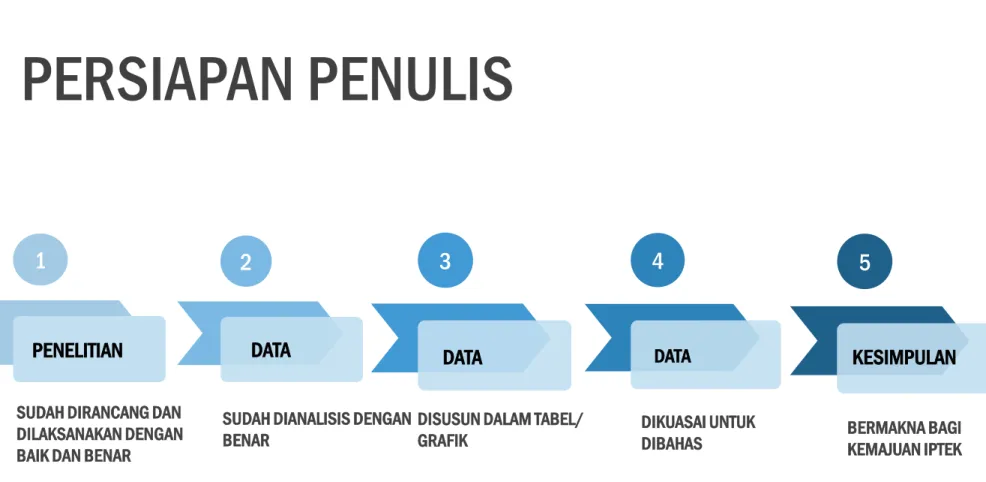
1
PENELITIAN
2
DATA
3
DATA
4
DATA
5
KESIMPULAN
SUDAH DIRANCANG DAN DILAKSANAKAN DENGAN BAIK DAN BENAR
SUDAH DIANALISIS DENGAN BENAR
DISUSUN DALAM TABEL/
GRAFIK DIKUASAI UNTUK
DIBAHAS BERMAKNA BAGI
KEMAJUAN IPTEK
PERSIAPAN PENULIS
PETUNJUK UNTUK PENULIS
FORMAT PENULISAN
SESUAI JENIS ARTIKEL ILMIAH TIDAK DIIKUTI
TARGET PENULIS DAPAT TERTUNDA BELUM DAPAT DIPROSES
DIKEMBALIKAN UNTUK DIPERBAIKI.
1 2 3
JENIS
ARTIKEL ILMIAH
ORIGINAL ARTICLE
REVIEW ARTICLE
RESEARCH COMMUNICATION
SHORT REPORT/LAPORAN KASUS
4
5 COMMENTARIES/ULAS BALIK
6 CORRESPONDENCE
7 8
EDITORIAL
RAPID RESPONSE- E-letter
ORIGINAL ARTICLE
Syarat umum:
• Total < 4500 kata, biasanya 3000 kata (diluar abstrak, tabel, gambar, daftar pustaka)
• < 5 tabel atau gambar
• < 40 daftar pustaka
• Abstrak terstruktur (IMRAD)
• Abstrak < 300 kata
• Kata kunci 3-5
11
12
13
REVIEWS ARTICLE (Tinjauan Pustaka)
Yaitu :
Sistematic reviews dan meta analisis berdasarkan bukti (Evidence based)
Mencakup metode yang mendeskripsikan:
- Cara pencarian jurnal (searching) - Cara analisis
- Cara membuat ringkasan (summary) Syarat umum:
• Total < 5000 kata
• < 5 Tabel/gambar
• < 60 daftar pustaka
• Bila narasi artikel tinjauan pustaka sudah umum diketahui,
maka kurang menarik dan cendrung tidak diterima untuk
publikasi
16
17
Short Report (Laporan Kasus)
20
Syarat umum:
• Total < 1500 kata
• brief abstract (< 250 words), IMRAD
• 1 tabel atau gambar
• Maksimum 12 daftar pustaka
• Ada kotak summary < 5 pesan penting (main massages)
• Ada kotak kebijakan < 3 implikasi kebijakan
• Format: Introduction, Case report, dan Discussion
Occup Environ Med 2003; 50: 696-698
Can salivary lead be used for biological monitoring of exposed persons ?
D Koh, V Ng, LH Chua, Y Yang, HY Ong, SE Chia
Correspondence
22
Syarat umum:
• Respon untuk artikel yang telah dipublikasi
• <300 kata
• < 6 daftar pustaka
• Penulis menyatakan tidak ada konflik kepentingan (competing interest)
• We are especially interested in letters to editor that relate to
recent journal content and which help readers to interpret and
place it in context
23
Commentaries
Publikasi dari komentar artikel minimal terdiri dari 500-600 kata
Membahas hal-hal penting dari artikel tersebut
Memuat hal-hal baru dan topik yang menarik
24
25
Research Communication
Yaitu komunikasi antar peneliti membahas suatu topik
tertentu yang dipublikasi dalam bentuk tulisan ilmiah
26
• Editorials dan Leaders adalah Kelompok penilai (peer- reviewed) sebelum artikel diterima
• Biasanya dalam suatu komisi penilai, but unsolicited submissions also considered
We are keen to consider contributions, or ideas for contributions, from a broad international authorship
Editorial and Leader
J Sng, D Koh.
Nanocommentary: Occupational and environmental health and nanotechnology – what’s new ?
Occupational Medicine 2008; 58: 454-455.
Rapid Responses
29
• Rapid responses adalah respon cepat dari pembaca suatu artikel tertentu yang dipublikasi melalui suatu website yang dikirim ke editor
• Kontribusinya terhadap abstrak atau atau isi artikel secara keseluruhan dalam bentuk pertanyaan.
• Letaknya pada kanan atas artikel ada tulisan kotak isi (“contents box”)
• Klik pada tulisan “e-Letters: dan kirim respon paper kita ke link artikel tersebut
• Tujuannya untuk mempublikasi semua respon cepat dari artikel
tertentu di website dalam 7 hari setelah diterima
NEWS EXTRA: Andrew Cole
Two thirds of doctors in UK say the NHS could not cope with bird flu epidemic BMJ 2006; 333: 674-a [Full text]
Gerald C H Koh, Assistant Professor Yong Loo Lin School of Medicine, National University of Singapore, David Koh Send response to journal:
Re: Preparedness for a Bird Flu Pandemic:
Comparing UK and Singapore’s Healthcare System
It is with great interest that we read the article in BMJ by Coles who reported the preparedness of a thousand-over UK doctors for a bird flu epidemic.(1) We are currently surveying our local healthcare workers (HCWs) on their preparedness for a bird flu pandemic and would like to share our preliminary findings. To date, 1,812 healthcare workers from our public healthcare system: one tertiary hospital, two community hospitals and 9 GP polyclinics have participated in our survey, with an overall response rate of 84.4%. Although our survey’s questions were not identical to the ones in the BMJ article, it included similar questions that allow some comparison. The following compares the questions and response percentages between Cole’s article and our study (it must be noted that the UK survey was conducted only on doctors whereas we included healthcare workers from all disciplines and occupations):
UK - 1. NHS cannot cope with an influenza pandemic = 68%
2. Personally prepared for an avian influenza pandemic = 22%
3. Personally badly or very badly prepared for an avian influenza pandemic = 37%
4. Not received any information from Department of Health or their trust about planning for an avian influenza = 56%
Singapore
1. Disagree that my healthcare institution is prepared for an avian influenza pandemic = 2% (N=35) 2. Agree that I am personally prepared for a bird flu pandemic = 70% (N=1264)
3. Disagree or strongly disagree that I am personally prepared for a bird flu pandemic = 10% (N=180) 4. My institution has not informed me of their bird flu outbreak preparedness plan = 9% (N=169)
We did not ask whether they know about the virology and progression of bird flu. Instead, we administered a twelve-question bird flu knowledge test on all participants and found that 90% of respondents got more than half the questions correct. We also did not ask whether they had made sufficient personal preparations but had asked whether they had participated in bird flu preparedness training or activities in the past 6 months.
72% had attended infection control training and 60% had participated in infection control audits. 76% had received influenza vaccination and 80%
have received training in the use of personal protective equipment (PPE). There could be several reasons for these differences in responses.
Singapore managed a SARS outbreak in 2003 and the experience has led to our citizens becoming more vigilant and healthcare workers more prepared for an infectious disease outbreak. Moreover, experts believe that a bird flu pandemic would most likely arise from East Asia and although Singapore does not have any live poultry industries, it expects to be affected early when it occurs.(2) To be prepared for an avian influenza pandemic, our local Ministry of Health has issued public and healthcare bird flu preparedness plans, audited healthcare institutions on their bird flu contingency plans, built extra isolation rooms in designated hospitals, encouraged influenza vaccination of healthcare workers and patients at risk, and stockpiled PPE and Tamiflu®.(3) We must also take into consideration that various healthcare institutions may have different levels of preparedness for a bird flu outbreak. We found from our data that HCWs from community hospitals were less prepared, had more misconceptions about bird flu transmission and PPE use, and were less concerned about bird flu than tertiary hospital HCWs.(4)
Scientists have concluded that it is possible to avert a global bird flu pandemic if human to human transmission is detected early and disease containment at the epicentre is effective.(5,6) To assess how prepared Asian countries are in managing a bird flu outbreak, we are currently collaborating with colleagues in Indonesia and Japan to conduct the survey. We welcome researchers from other Asian countries who are interested to collaborate to contact us. Dr Gerald C H Koh (Email: [email protected]), Dr David Koh
References:
1. Cole A. Two thirds of doctors in UK say the NHS could not cope with bird flu epidemic. BMJ 2006;333:674. (doi:10.1136/bmj.333.7570.674-a) 2. Day M. East Asia is most at risk of human flu epidemic, experts say. BMJ 2005;331:921.
3. Ministry of Health (Singapore). Influenza Pandemic Readiness and Response Plan. Dec 2005, Singapore (http://www.flu.gov.sg/resources/Readiness_Response _Plan_2005.pdf).
4. Koh GCH, Lee HY, Tan BY, Chan KM, Koh D. Comparison of preparedness, knowledge, attitudes, beliefs and concerns of healthcare workers between community hospitals and a tertiary hospital.
Poster presentation at 15th World Organisation of Family Doctors Asia-Pacific Regional Conference, Bangkok, 6-8 Nov 06.
5. Ferguson NM, Cummings DAT, Cauchemez S, Fraser C, Riley S, Meeyai A, Iamsirithaworn S, Burke DS. Strategies for containing an emerging influenza pandemic in Southeast Asia. Nature 2005;437/8:209-214. (doi:10.1013/nature04017.)
6. Longini IM, Nizam A, Xu S, Ungchusak K, Hanshaoworakul W, Cummings DAT, Halloran ME. Containing pandemic influenza at the source. Science 2005;309:1083-7.
Competing interests: None declared
Rapid Responses: Submit a responseto this article
Rapid Responses published:
Preparedness for a Bird Flu Pandemic: Comparing UK and Singapore’s Healthcare System
Gerald C H Koh, David Koh (6 October 2006)
thank
y o u !