Journal of Life Sciences
Volume 8, Number 8, August 2014 (Serial Number 76)
David Publishing Company www.davidpublishing.com
Publication Information
Journal of Life Sciences is published monthly in hard copy (ISSN 1934-7391) and online (ISSN 1934-7405) by David Publishing Company located at 240 Nagle Avenue #15C, New York, NY 10034, USA.
Aims and Scope
Journal of Life Sciences, a monthly professional academic journal, covers all sorts of researches on molecular biology, microbiology, botany, zoology, genetics, bioengineering, ecology, cytology, biochemistry, and biophysics, as well as other issues related to life sciences.
Editorial Board Members
Dr. Stefan Hershberger (USA), Dr. Suiyun Chen (China), Prof. Dr. Fadel Djamel (Algeria), Dr. Francisco Torrens (Spain), Dr. Filipa João (Portugal), Dr. Masahiro Yoshida (Japan), Dr. Reyhan Erdogan (Turkey), Dr. Grzegorz Żurek (Poland), Dr. Ali Izadpanah (Canada), Dr. Barbara Wiewióra (Poland), Dr. Amanda de Moraes Narcizo (Brasil), Dr. Marinus Frederik Willem te Pas (The Netherlands), Dr. Anthony Luke Byrne (Australia), Dr. Xingjun Li (China), Dr. Stefania Staibano (Italy), Prof. Dr. Ismail Salih Kakey (Iraq), Hamed Khalilvandi-Behroozyar (Iran).
Manuscripts and correspondence are invited for publication. You can submit your papers via Web Submission, or E-mail to [email protected] or [email protected]. Submission guidelines and Web Submission system are available online at http://www.davidpublishing.com.
Editorial Office
240 Nagle Avenue #15C, New York, NY 10034, USA
Tel: 1-323-9847526, 1-302-5977046; Fax: 1-323-9847374, 1-323-9080457 E-mail:[email protected], [email protected]
Copyright©2014 by David Publishing Company and individual contributors. All rights reserved. David Publishing Company holds the exclusive copyright of all the contents of this journal. In accordance with the international convention, no part of this journal may be reproduced or transmitted by any media or publishing organs (including various websites) without the written permission of the copyright holder. Otherwise, any conduct would be considered as the violation of the copyright. The contents of this journal are available for any citation. However, all the citations should be clearly indicated with the title of this journal, serial number and the name of the author.
Abstracted / Indexed in
Database of EBSCO, Massachusetts, USA Chemical Abstracts Service (CAS), USA
Database of Cambridge Science Abstracts (CSA), USA Database of Hein Online, New York, USA
Ulrich’s Periodicals Directory, USA Universe Digital Library S/B, Proquest
Chinese Database of CEPS, American Federal Computer Library center (OCLC), USA China National Knowledge Infrastructure, CNKI, China
Chinese Scientific Journals Database, VIP Corporation, Chongqing, China Index Copernicus, Index Copernicus International S.A., Poland
Google Scholar (scholar.google.com)
Subscription Information
Price (per year): Print $420, Online $300, Print and Online $560.
David Publishing Company
240 Nagle Avenue #15C, New York, NY 10034, USA
Tel: 1-323-9847526, 1-302-5977046; Fax: 1-323-9847374, 1-323-9080457 E-mail: [email protected]
David Publishing Company www.davidpublishing.com
JLS
Journal of Life Sciences
Volume 8, Number 8, August 2014 (Serial Number 76)
Contents
Pathology and Laboratory Medicine
633 Diagnostic Value of Hepatic Enzymes, Triglycerides and Serum Proteins for the Detection of
Hepatic Lipidosis in Chelonoidis carbonaria in Captivity
Gustavo Henrique Pereira Dutra
640 Individual Care Pathways in the Context of Complex Therapeutic System—Therapeutic Model
and Case Report
Kálmán Erdélyi
648 A Comparative Study on Feeding Practice and Nutrition Status among 6-23 Months Age Children
Taslima Khatun, Md Shahjahan Matabbar, Manika Rani Sarker, Asad-Ud-Daula and Asirul Hoque
Botany and Zoology
660 Effect of Salinity Stress and Mutagenic Sodium Azide on Callus Induction and Plant Regeneration
of Borage (Borago officinalis) in Vitro
Al-Mohammed Maher H. S., El-Kaaby Ekhlas A. J., Al-Anny Jenan A. and Musa Abdul-kadhim J.
668 Effect of Fermentation on Nutrient and Anti-nutrient Composition of Millet (Pennisetum glaucum)
and Soyabean (Glycine max) Blend Flours
Anthony Ojokoh and Babatunde Bello
676 Toxic Effects of Seed Methanolic Extracts of Endemic Albizia Species (Fabaceae) from
Madagascar on Animals
Hanitra Ranjàna Randrianarivo, Anjarasoa Ravo Razafindrakoto, Holy Christiane Ratsimanohatra,
Lovarintsoa Judicaël Randriamampianina, Clara Fredeline Rajemiarimoelisoa, Lolona Ramamonjisoa, David Ramanitrahasimbola, Danielle Aurore Doll Rakoto and Victor Louis Jeannoda
690 Distribution of Origanum vulgare L. and Population Dynamics During the Last Decade in
Armenia
699 Economic and Market Analysis of Swine Rearing and Pork Production in Ghana
Kwamina Ewur Banson, Josephine Nketsia-Tabiri, Kweku Anno and Emmanuel Kofi Dagbui
709 Challenges in Forensic DNA Profiling and Critical Issues in Interpretation of STR Profiles
Seah Lay Hong
716 Physico-chemical and Bacteriological Specification Groundwater of Tangier
Journal of Life Sciences, ISSN 1934-7391, USA
Diagnostic Value of Hepatic Enzymes, Triglycerides and
Serum Proteins for the Detection of Hepatic Lipidosis in
Chelonoidis carbonaria
in Captivity
Gustavo Henrique Pereira Dutra
Aquário Municipal de Santos, Avenida Bartolomeu de Gusmão sn Ponta da Praia-Santos-SP, 11030-500, Brazil
Received: June 18, 2014 / Accepted: August 15, 2014 / Published: August 30, 2014.
Abstract: Hepatic lipidosis is a common lesion in chelonians and may be related with vitellogenesis, hyperparathyroidism, follicular stasis, fatty diets or lacking nutrients, sedentary life and obesity, bacterial toxins in liver and starvation. Clinical signs are unspecific. Routine biochemical tests don’t have specificity and it is better defined through biopsy. The objective was evaluated the biochemical hepatic profile of red footed tortoises (Chelonoidis carbonaria) with the histopathological findings of lipidosis by laparoscopic biopsy. Samples of blood were collected for biochemistry of thirty-six animals from two different groups, twenty animals from a zoo and sixteen from a breeder. The animals were submitted to liver biopsy by videolaparoscopy. Three fragments were collected, two of them were processed by histology and one went to electron microscopy. Nineteen tortoises from the zoo had lipidosis in laparoscopy and macrovesicular degeneration. Fifteen tortoises from the breeder had microvesicular degeneration. The diagnosis of steatosis was confirmed by electron microscopy. There was no statistical difference of aspartate aminotransferase levels between the two groups; however there was significant difference of triglycerides levels. The enzymatic activity of transaminases is not related to the histological grading of lipidosis in tortoises, however triglycerides levels are higher in animals with more severe gradation.
Key words: Biopsy, steatosis, liver, Chelonoidis, enzymes.
1. Introduction
The chelonian liver acts in the metabolism of lipids, glycogen and protein [1]. It is responsible by the degradation of nucleotides for uric acid excretion, and acts as the main storage of fat in the body. Its functions may change during events such as hibernation and reproduction in females, when vitellogenesis and protein synthesis increase, and the liver may be larger and with changes in color and texture [2]. Such variations are important differentials for primary or secondary liver diseases.
Steatosis or hepatic lipidosis represents the excessive and abnormal accumulation [3] of lipids (triglycerides) within the hepatocyte [4-6]. There
Corresponding author: Gustavo Henrique Pereira Dutra, DVM, research field: experimental and comparative pathology. E-mail: [email protected].
are two fundamental types of steatosis: macrovesicular and microvesicular [7-11].
Liver enzymes are known markers of hepatocellular damage and cholestasis, but are nonspecific in indicating the causes of the pathological states and interpretation can be challenging due to presence of isoenzymes and different causes of induced activity. More definitive diagnosis are often only reached on biopsy [12-14], and in chelonians it is invasive, through the inguinal fossa [15] often by videolaparoscopy.
Clinical signs, hematological and biochemical variations are often nonspecific. Tests of biliary function have not been validated in chelonians. Lipidosis indicators also include cholesterol and triglycerides [16].
The objective of this work was to evaluate the
D
diagnostic value of hepatocellular damage and cholestasis enzymes activity, triglycerides, and basic serum protein profile for the diagnostic of hepatic lipidosis in red footed tortoise (Chelonoidis carbonaria, SPIX, 1824).
2. Materials and Methods
A total of 36 red footed tortoises (Chelonoidis carbonaria, SPIX, 1824) were assessed. Twenty animals (11 males and 9 females) were from “Fundação Parque Zoológico de São Paulo” (São Paulo Zoo) and sixteen (8 males and 8 females) were from a commercial breeder. The tortoises from the Zoo had a protein-rich diet (ground beef, sardines and boiled egg) that was offered in alternate days, and daily, they were fed pumpkin, carrot, banana, apple and papaya and dark greens. The tortoises from the breeder were fed vegetables, greens and fruits daily.
This experiment was approved by the Diretoria de Ecossistemas do Instituto Brasileiro do Meio Ambiente e dos Recursos Naturais Renováveis (Environmental Brazilian Agency; license 30/2002, process 02027.003103/02-49) and by the University of São Paulo, College of Veterinary Medicine, Internal Animal Care and Use Committee. Before the studies all the animals were fasted for 24 h in a temperature controlled room (27 ºC to 32 ºC). The animals had an average weight of 3.6 kg.
The chelonians were washed with povidine-iodine degerming with polyvidone iodine at 10% (Laborioide degermante®, Segmenta, Ribeirão Preto-SP, Brazil), sedated with ketamine hydrochloride (Dopalen®, 100 mg/mL, Vetbrands Jacarei-SP-Brazil) dosage of 60-80 mg/kg intramuscularly. Five milliliters blood aliquots were then collected via jugular or coccygeal vein, and the serum was immediately cooled at 4 ºC.
The serum samples were analyzed in a semi-automatic biochemical analyzer with variable wavelength filter, Bio 2000 (Bioplus® São Paulo, SP, Brazil) for AST, ALT, ALP, GGT activities; and triglycerides, total proteins and albumin from
Laborlab® (Laborlab® Guarulhos, SP, Brazil) at 37 ºC.
Core biopsies (measuring two centimeters by two millimeters) of hepatic tissue were collected with a semi-automatic guillotine biopsy cutting needle (gauge 15) TEMNO® (Allegiance Healthcare Corporation McGaw Park, USA), and images of the hepatic surface were taken using the laparoscopic probe. After intubation and anesthesia with isoflurane (Forane® Abbott, São Paulo, SP, Brasil), the animals were placed in dorsal recumbence and a surgical access was opened through the right inguinal fossa, through a small incision through which was introduced a five millimeters laparoscopic probe Olympus® (Olympus Optical Medical do Brasil-São Paulo-SP Brazil), under halogen light.
Two hepatic fragments from each animal were submitted to histological processing for hematoxylin and eosin, Masson’s trichrome, and Periodic acid-shiff staining. A third fragment was fixed in glutaraldehyde at 2% for ultrastructural study. The contrast of the ultra-thin slices of about 90 nm was given by uranyl acetate at 2% and lead citrate. The electro micrographs were obtained in electronic microscopy of transmission Philips EM-201C (Koninklijke Philips Eletronics®, Amsterdam, Netherlands).
The statistical analysis was done using Biostat for Windows 2009® (Analystsoft® Inc, USA). The Kolmogorov-Smirnov’s test was applied to verify that the curve assumed a Gaussian distribution. A two-tailed t test was used for average comparison of each biochemical evaluation and independent samples were compared using the Mann-Whitney’s test.
3. Results
The data regarding biochemical serum analysis of animals from the Zoo are grouped in Table 1 and from the breeder in Table 2.
There was no need of pneumocoelom for
Table 1 Serum biochemical values of red footed tortoises of zoo, Sao Paulo, 2003.
Gender AST
σ 1.5786 0.1424 0.2724 0.0145 0.2724 13.873 6.8087 11.334 0.3964
SEM 0.353 0.0318 0.0609 0.0033 0.0609 3.1022 1.5225 2.5345 0.0886 variance 2.4919 0.0203 0.0742 0.0002 0.0742 192.4711 46.3579 128.4711 0.1571 AST (Aspartate aminotransferase); ALT (Alanine aminotransferase); TG (triglycerides); GGT (γ-glutamil transferase); ALP (Alkaline Phosphatase); TP (Total Protein); Alb (Albumin); Glob (Globulin) A/G (Albumin/Globulin Ratio); SD—standart deviation (σ); SEM—standart error of mean.
Table 2 Serum biochemical values of red footed tortoises of breeder, Sao Paulo, 2003.
Gender AST
quickly solved by the natural hemostatic process. There was no death during the experimentation.
Tortoises from the breeder had laparoscopy images of hepatic lobes slightly rounded and of magenta color. One animal had liver wine-colored, soft consistency, tapered edges, not easily pervious to the entry of the needle bevel (Figs. 1 and 2). The great majority of testudine from breeder evidenced severe microvesicular degeneration consistent with glycogen accumulation or hydropic degeneration, with no associated inflammation or fibroplasia. In animal number 11 from breeder, was observed a preserved histological hepatic architecture, with healthy hepatocytes (Fig. 4), abundant amount of glycogen and none fibroplasia evident in the Masson´s trichrome.
The laparoscopic image of the 19 tortoises from São Paulo Zoo were consistent with fatty liver disease, with rounded edges, brownish yellow color, unctuous aspect of surface and friable (Fig. 3). The tortoise number 5 had a liver with preserved dimensions, magenta color and soft consistency. After the sampling, the samples were placed in test tubes and almost all of them floated in aqueous solution of formalin.
After microscopic review, 16 tortoises from the zoo had macrovesicular degeneration consistent with lipid accumulation, with eccentric nuclei, but with no inflammation or fibrosis. In tortoise number 5 from the zoo, a mild microvesicular degeneration was observed. In two animals from the zoo, steatosis was observed throughout the cut length, with heterophilic and mononuclear inflammation (Fig. 5), one of them with mild fibroplasia and the second with marked fibrosis and macrovesicular degeneration (Fig. 6). Ultrastructure evaluation of the all animals from the zoo had electrodense vacuoles typical of lipid droplets (Figs. 7 and 8).
4. Discussion
The open circuit (non-rebreathing) of anesthesia was enough in this study for tortoises up to 5.0 kg for the technique of hepatic biopsy by coelomic access.
The access used for the biopsy by the inguinal fossa allowed clear observation and sampling of specimens, according to previous works for videolaparoscopy in chelonians [15, 17, 18]. Contrary to the proposed by Divers, Stahl and Camus, 2010 [19], even without the use of pneumocoelom, there was quality on liver visualization.
Fig. 1 Laparoscopic image of a normal liver of red footed tortoise.
Fig. 2 Normal left lobe liver biopsy of tortoise.
Fig. 4 Normal histology of tortoise liver HE 400 ×.
Fig. 5 Microvesicular steatohepatitis of red footed tortoise liver HE 400 ×.
Fig. 6 Hepatic fibroplasias in tortoise liver showing collagen fibers (blue staining) and melanin pigment, common in reptile liver. Masson’s trichrome 400 ×.
There was no statistical difference on AST activity between the two groups (t = 1.2297 and P = 0.2273), or between female and male (p = 0.8702 and t = 0.1657, tc = 2.1009), in disagreement with Christopher et al. (1999) [2]. Testing AST activity may have a low
Fig. 7 Transmission electron micrograph showing electrodense droplets of fat in the cytosol of hepatocyte. Osmium tetraoxide 6000 ×.
Fig. 8 Transmission electron micrograph showing inflammatory cell in hepatic parenchyma of tortoise. Osmium tetraoxide 6000 ×.
sensitivity for diagnosing chronic fibroblastic injury, where there are fewer hepatocytes, since they are replaced by connective tissue. Also, ALT activity was not statistically between the two groups (t = 1.4401 and p = 0.159; α = 0.05). These findings were similar to what other found for AST and ALT activities [2, 16, 20].
p = 0.0634; α = 0.05), once more there was a lack of analytical sensitivity of the test, with low activity for the zoo animals and readings bellow the detectable limit for the breeder’s group. Although the steatosis pathophysiology involves cytosolic and mitochondrial damage [3-6], which often lead to enzymatic extravasation or induction of production, the results of the enzymatic activities only revealed that AST activity was the enzyme with more analytical sensitivity in tortoises, with low diagnostic specificity for hepatic steatosis gradation. Similarly, others also found this in other tortoises [2, 16, 20]. Concentrations of TP were significantly different between the two groups (t = 5.9916 and p < 0.0001; α = 0.05) with TP levels from the zoo tortoises being higher than from the breeder ones. These findings were likely due to the protein rich diet of the zoo tortoises. The TP differences were likely due to albumin concentration that was significantly higher in the animals from the zoo (t = 3.7079 and P = 0.0007;
α = 0.05). These differences also leaded to a significantly higher albumin to globulin ratio in the zoo’s tortoises (t = 2.0557 and P = 0.0476; α = 0.05). These findings suggest that although there were macroscopic and microscopic findings consistent with steatosis in the animals from the zoo, there was no apparent loss in hepatic production of albumin. This is unexpected since steatosis is knowingly a cause of hepatic insufficiency that could lead to decreased albumin production [3, 12]. Albumin has a small role in colloid osmotic pressure of chelonians, approximately 20%. Very little is known about the transport capacity of albumin in chelonians, the major part of proteins are alpha-1 and alpha-2 globulins, transferrins, lipoproteins, fibrinogen, isoagglutinins (globulins) and vitelline [1], which question the clinical impact of our findings.
The tortoises with more severe liver disease (from zoo) had significantly higher concentrations of triglycerides (t = 4.7756 and P < 0.0001; α = 0.05) than the ones from the breeder. Triglycerides may be
good biomarkers for hepatic lipidosis, or severe liver disease of other etiologies in tortoises. Prior works showed that hypertriglyceridemia can also be seen females with follicular stasis or in vitellogenesis had higher levels of triglycerides [2, 21, 22]. In this work, the differences on levels of triglycerides between males and females were seemingly random.
The mild fibroplasia and heterophilic and mononuclear inflammation observed in two animals from the zoo, appeared to be a progression to cirrhosis [7-11, 23]. The presence of the Mallory’s hyaline corpuscle, one of the criteria suggested in classification of steatohepatitis, was not observed in any of the samples collected from tortoises. The histopathological findings of microvesicular liver degeneration and macrovesicular lipid accumulation, was also used as prognosticators by others [7-11, 20, 25], as the microvesicular degeneration findings, without associated inflammation or fibrosis is considered a mild pathogenic process, according with gradation system previously proposed [7-11, 24, 25]. The presence of lipid was confirmed by transmission electronic microscopy. Since no differences were found between males and females in any of the tests, vitellogenesis was considered an unlikely confounder, and the nutrition was the probable etiology of the differences between groups [7, 26, 27].
5. Conclusions
Although there was no correlation between the activity of hepatic transaminases measured in the serum of red-footed tortoises and hepatic steatosis caused by hypercaloric diet, the serum triglyceride levels appeared to be reliable markers of hepatic lipidosis or severe hepatic disease.
References
[1] Dessauer, H. C. 1970. “Blood Chemistry of Reptiles: Physiological and Evolutionary Aspects.” In Biology of the Reptilia, edited byGans, C. London: Academic Press.
Hematologic and Biochemical Values of Free Ranging Desert Tortoises in the Mojave Desert.” Journal of Wildlife Diseases 35 (2): 212-238.
[3] Herdt, T. 1993. “Digestão e Absorção: os Processos Não Fermentativos.” In Tratado de Fisiologia Veterinária, edited by Cunningham, J. G. Rio de Janeiro: Guanabara-Koogan Editora.
[4] Fabris, V. E. 1992. “Lesões Celulares Reversíveis e Irreversíveis.” In Patologia, Processos gerais, edited by Montenegro, M. R., and Franco, M. São Paulo: Livraria Atheneu Editora.
[5] Cotran, R. S., Kumar, V., and Robbins, S. L. 1996. “Lesão celular e Morte Celular.” In Patologia Estrutural e funcional de Robbins, edited by Cotran, R. S., Kumar, V., and Robbins, S. L. Rio de Janeiro: Guanabara-Koogan Editora.
[6] Crawford, J. M. 1996. “Fígado e Vias Biliares.” In Patologia estrutural e Funcional de Robbins, edited by Cotran, R. S., Kumar, V., and Robbins, S. L. Rio de Janeiro: Guanabara-Koogan Editora.
[7] Mezey, E. 1999. “Fatty liver.” In Schiff's Diseases of Liver, edited by Schiff, E. R., Sorrel, M. F., and Madrey, W. C. Philadelphia: Lippincott, Willians and Wilkins. [8] Bianchi, L. 2001. “Liver Biopsy in Elevated Liver
Function Tests? An Old Question Revisited.” Journal of Hepatology 35: 290-294.
[9] Mincis, M. 2002. “Esteatose e Esteatohepatite Não Alcoólicas.” In Gastroenterologia e Hepatologia- diagnóstico e Tratamento, edited by Mincis, M. São Paulo: Lemos Ed.
[10] Parise, E. R. 2002. “Esteatose Hepática.” Atheros 13: 52-55.
[11] Sanyal, A. J. 2002. “AGA Technical Review on Nonalcoholic Fatty Liver Disease.” Gastroenterology 123 (5): 1705-1725.
[12] Sherlock, S. 1998. “Avaliação da função hepática.” In Doenças do Fígado e Sistema Biliar, edited by Sherlock, S. Rio de Janeiro: S. Guanabara Koogan. [13] Alves, Y. A. F., Gayotto, L. C. C., and Carrilho, F. J.
2000. “Anatomia Patológica das Hepatites por Vírus.” In Centro de Vigilância Epidemiológica. Manual de Vigilância Epidemiológica—Hepatites Virais, Normas e Instruções, São Paulo: Secretaria do Estado da Saúde. [14] Tostes, R. A., and Bandarra, E. P. 2002. “Biópsia
Hepática em Cães: Relação Entre a Qualidade da Amostra e Grau de Conclusão do Diagnóstico.” Arquivo Brasileiro de Medicina Veterinária e Zootecnia 54 (5): 468-472.
[15] Taylor, W. M. 2006. “Endoscopy.” In Reptile Medicine
and Surgery, edited by Mader, D. R. Saint Louis: Saunders Elsevier.
[16] Hernandez-Divers, S. J., and Cooper, J. E. 2006. “Hepatic Lipidosis.” In Reptile Medicine and Surgery, edited by Mader, D. R. Saint Louis: Saunders Elsevier.
[17] Hernandez-Divers, S. J. 1988. “An introduction to reptile endoscopy.” In Proceedings of the 5th Annual Conference, Association of Reptilian and Amphibian Veterinarians.
[18] Divers, S. J. 1997. “A Clinician’s Approach to Liver Diseases in Tortoises.” In Proceedings of the 4th Annual Conference, Association of Reptilian and Amphibian Veterinarians.
[19] Divers, S. J., Stahl, S. J., and Camus, A. 2010. “Evaluation of Diagnostic Coelioscopy Including Liver and Kidney Biopsy in Freshwater Turtles (Trachemys scripta).” Journal of Zoo and Wildlife Medicine 4: 677-687.
[20] Jacobson, E. R., Schumacher, J., Telford, S. R., and Greiner, E. C. et al. “Intranuclear Coccidiosis in Radiated Tortoises (Geochelone radiata).” Journal of Zoo and Wildlife Medicine 25 (1): 95-102.
[21] Frye, F. L. 1991. “Common Pathologic Lesions and Disease Process.” In Reptile Care, An Atlas of Diseases and Treatments, edited by Frye, F. L. Neptune City: v2. TFH Publications.
[22] McArthur, S. 2004. “Problem Solving Approach to Common Diseases of Terrestrial and Semi-Aquatic Chelonians.” In Medicine and Surgery of Tortoises and Turtles, edited by McArthur, Wilkinson, R., and Meyer, J. Oxford: S. Blackwell Publishing.
[23] Guedes, R. M. C., and Lavalle, G. E. 2004. “Hepatic Cirrhosis in a Red-foot Tortoise (Geochelone carbonaria) A Case Report.” Arquivo Brasileiro Medicina Veterinária e Zootecnia 56 (1): 123-125.
[24] Divers, S. J., and Cooper, J. E. 2000. “Reptile Hepatic Lipidosis.” Seminars in Avian and Exotic Pet Medicine 9: 153-164.
[25] Hernandez-Divers, S. J., and Cooper, J. E. 2001. “Reptile Hepatic Lipidosis.” In Proceedings of the Annual Conference, Association of Reptilian and Amphibian Veterinarians.
[26] Gentile, L. B., and Ferreira, A. M. R. 1996. “Lipidose Hepática Idiopática Felina.” Clínica Veterinária 1 (3): 8-13.
Journal of Life Sciences, ISSN 1934-7391, USA
Individual Care Pathways in the Context of Complex
Therapeutic System—Therapeutic Model and Case
Report
Kálmán Erdélyi
Újpest Mentalhygienic Outpatient Center, 40-42 Nyár Street, Budapest 1041, Hungary
Received: July 16, 2014 / Accepted: August 12, 2014 / Published: August 30, 2014.
Abstract: Acomplex multifactorial therapeutic system was established and developed during the past three years. Here present the basic approach and the individualized therapeutic strategies of this therapeutic system by examples of specific case reports. The aim of the study is to point out to the real mission of our outpatient care, namely psycho-social reintegration that is achieved by a therapy with a unique pattern. Case reports: 1. A 59-year-old female patient suffering from psychosomatic muscular tension, which started two years ago. After a partially effective cognitive-behavioral therapy a severe traumatic event in the patient’s past in connection with the symptoms was revealed, then the trauma was processed via psychodynamic approach. 2. A 56-year-old female patient suffering from psychosomatic symptoms and depression went through a therapeutic healing process, which focused on the development and maturation of her personality (from a “child” to an “adult”). Conclusion: All the processes of the complex group-centered dynamic therapy proved more effective compared to the classic static relationship between the psychiatrist and the patient. The multifocal therapy is appreciated more and more in parallel to the experiences gained, making it easier to establish and strengthen the therapeutic alliance. The patients have positive feelings about the help given and the possibilities offered. The author’s therapeutic team is appreciated by the patients and they regard the author’s center as a peaceful location of their lives being under cover, where voluntarily and willingly they can participate in the individualized therapy with great success.
Key words: Complex multifactorial system, individualized therapy, psycho-social reintegration.
1. Introduction
It is considered that the fundamental tasks of the outpatient therapeutic work to reach a level of stabilization by building a bio-psycho-social unit that create optimal conditions. The main aim is the psycho-social reintegration achieving optimal state level and returning patients to their productive lives in the community. Prevention, acute, chronic care and therapy together with the stabilization of the compensated state, that means relapse prevention, are the basic tasks. Prevention means to decrease the onset (incidence), the duration (prevalence) and the
Corresponding author: Kálmán Erdélyi, M. D., research fields: psychiatric rehabilitation, social reintegration through complex therapeutic approach. E-mail: [email protected].
residual disability of mental disorders [1]. Leaving the classic static therapeutic model behind, a new system with dynamic approach, integrative therapeutic orientation has been developed. The multifactorial system has become more colorful in a way like this. All the specialists of the team, namely psychiatrists, psychologists, art therapist, social therapist and the nursing staff have their own roles, tasks and responsibilities. The team members cooperate with each other placing the major problems, actualities of the patients in the centre of interest. The author’s team work is characterized by the following sentence: System inside the system. The process of the patient care with professional cooperation makes it easier to direct the patients to the appropriate therapeutic way. Providing continuity of care and integrated services is
D
essential. To maintain the social network is a challenge, but can be successfully carried out by applying a systemic therapeutic structure. The complex, advanced special outpatient care allows a substantial proportion of the patients not to be removed from their home environments or workplaces and not giving up or losing their individual roles.
The population number of the district the author’s outpatient center functions is about 100,000. The annual number of the attendance was 14,264 in 2013. Different types of the individual psychotherapy, group psychotherapy, art therapy and social therapy are used according to the basic problem and the current state of the patient, with or without pharmacotherapy. The community-like service with different therapeutic modalities has the capacity for 120-130 patients per week. Therapeutic options over the classic treatment (control, pharmacotherapy) are presented in short.
2. Patients and Methods
In the last three quarters of the year 172 patients (the number of the patient’s attendances was 1,304) participated in different psychotherapies, namely 74 patients (582 attendances) in individual-, 41 patients (393 attendances) in verbal group-, 37 patients (193 attendances) in stress management group psychotherapy and 20 persons (136 attendances) in autogenic training [2, 3]. Summary of the therapies performed by psychologists is presented in Table 1.
Art therapy [4, 5] means four groups and four
methods in the author’s outpatient center. Self-knowledge group is a closed, thematized and directed group with the aim improving self-knowledge, recognizing psychic obstructions. Group with emphasis on activity is an open, non-thematized and non-directed group practicing social relations, sharing experiences via common creative works mostly for schizophrenic patients. Free association group is an open, partially thematized and directed group with emotional involvement and sharing. Last but not least free creative work, namely Art Brut, an open, non-thematized, non-directed group, creative work with continuous conversation between the patients. Further joint purposes of art therapy are to reach and to keep in connection with the clients widely and also create a lively and extensive cooperation within the team in order to have effective therapy.
In the last year 59 patients took part in art therapies held once a week, the whole number of the attendances was 1,440. It should be noted that some of the patients are involved in more parallel art therapy sessions.
In a six-month period of 2013, six different social group therapies (Game—with the aim to reach a more balanced way of life discovering the joy of playing and mobilizing emotions; Psychoeducation; Living—means a complex management of unhealthy lifestyle and the purpose is to improve the patient’s quality of life and to make more conscious decisions in everyday life, mostly for schizophrenic patients; Art
Table 1 Summary of the psychological therapeutic modalities.
Individual therapy Verbal „free-association”
group therapy Autogenic training
Stress management group therapy
Content
Verbal elaboration and reframing of the client’s problems
Exploration of the internal context of psychological and interpersonal problems
12 steps structured excercises
Treatment of stress induced physiological, emotional, cognitive reactions
Purpose Fitting to the needs of the clients, individual goals
Adults with psychological and interpersonal problems
Adults suffering from anxiety disorders
Adults suffering from mental distress Form Two-participants situation Open verbal small group
Closed, small group structured in time (12 sessions) and method (relaxation practice)
therapy—creative techniques which help the patients to express their emotions; Literature; Literary group—lecture, talking, watching movies, discussion of novels and poems with the aim to be able to establish social contacts with group experience and improve self-knowledge and motivation) were started with 83 patients and they attended 602 times altogether.
Social skills therapy is very essential for the chronic schizophrenic patients [6]. Both art therapy, psychoeducation, group therapy and recreational activities, like common organized programs (visit to the museum, weekend trips) are very important to help the patients to be interested in each other and become able to contact each other step by step.
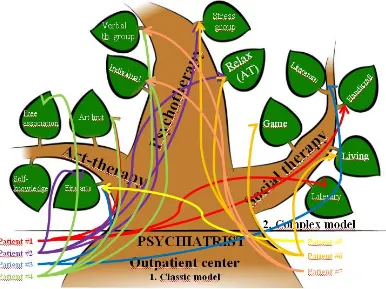
These above-mentioned therapeutic options ensure the complexity of the system and thus give the real chance to put the individualized care pathway into practice [7]. A tree diagram symbolizing both the classic and the patient-specific individualized model
by a multicolored, branchy tree with broad trunk is shown (Fig. 1).
3. Case Reports
Below the specific pattern of the unique therapeutic way is being demonstrated the specific pattern of the unique therapeutic way through specific cases, proving the advantages of this caring approach and practice, such as: 1. The voluntary, active latching on to the programs. 2. The connection of the patient into the care system through the experience of subjective usefulness. 3. The sense of security of the staff and the patients based on the fact, that a patient maintains the connection—by the needs of his condition: voluntarily and actively with the outpatient center and the therapeutic team.
M.I., a 59-year-old single woman (Fig. 1 Patient #4) was admitted to the author’s outpatient center suffering from psychosomatic trapezius muscular tension, which started two years ago. Awaking at
nights she usually found her hands firmly clenched. Formerly she had panic disorder effectively treated by pharmacotherapy. At the beginning of the therapeutic contact the author had a first impression, that she was a highly self-limited, inhibited lady, who had to make constant efforts to be appreciated by her actual milieu. Emotional stress was often associated with the prolonged contraction of neck muscles. Symptoms fluctuated over time and might have been most intense during periods of stress.
She was directed to the author’s psychologist, whose first therapeutic step was the cognitive therapy with the aim to attain relaxation practice and to improve coping skills. At the very beginning of the cognitive and behavior therapy it came to light that she had a car accident and had been suffering from the above-mentioned symptoms generated by that trauma. The therapist (the author’s psychologist) overcame the patient’s denial of the traumatic event, encouraged her to relax and removed her from the source of the stress, thus took the necessary steps to reduce the mental stress instead of leaving the process to be converted into somatic symptoms. The patient couldn’t recall the details of the incident, that’s why hypnotherapy was the second psychotherapic intervention. The patient in a hypnotic trance could recall memories and could describe an event with an intensity similar to that when it occured and experienced a sense of relief as a result. Her symptoms suddenly renewed and the psychotherapy became less efficient.
At this point she recalled another trauma from her past. At the age of 14 she became a victim of sexual violance, she was raped. The patient and the therapist worked together, aiming to resolve the problem and the patient actively participated in the treatment. All those therapeutic techniques, like suggestion and reassurance were aimed at decreasing the client’s anxiety.
Summarizing the above-mentioned after a partially effective cognitive-behavioral therapy a severe traumatic event in the patient’s past in connection with
the symptoms was revealed, then the trauma was processed via psychodynamic approach.
Having finished pharmacotherapy (SSRI and benzodiazepine) and psychotherapy held for one year, the client joined the “Group with Free Association” (art therapy) and participated in it regularly, once a week for one year. She associated drawing with self-knowledge. At the beginning she was somewhat disturbed and she put a question to herself: “I wonder who I am” (Fig. 2). Slowly she learned to express herself, her own feelings through her drawings, art works in front of the members of the group. She learned to accept herself. Pleasure and high-level expression characterized her creative activities.
The difficulties she experienced in the individual therapeutic process were drawn including her hope for a more pleasant future without any difficulties (Fig. 3).
The next group of art therapy she joined after a year was the “Self-knowledge Group” working with the aim to improve self-knowledge. It’s a closed, thematized, directed group with limited number of participants. In addition, due to the positive effects of drawing she joined another group, the free creative
Fig. 3 That’s my way. Step by step to the balance.
group “Art Brut” for drawing occasionally. After two years it was the first time the client was able to talk about the sexual violance she suffered from in front of people.
The patient had a look at herself from the window of a ship cabin: she became able to observe herself, her actual state, and her psychic, emotional actions from an outside perspective. The picture reflects an
intense feeling of solitude, though a compensatory coping mechanism seems to emerge: she can observe herself now from an outside, self-reflective perspective, which is essential for grounding her inner emotional stability (Fig. 4).
Now her mental state is stable. She finished pharmacotherapy two years ago and she has been drug-free since then. She is able to formulate exactly what she really wants and what she can do.
B.T.P, a 52 years old female patient (Fig. 1 Patient #2) suffering from psychosomatic symptoms and depression became engaged in therapy. She has been visiting the author’s outpatient center since January 2010 suffering from the above mentioned symptoms and demotivation. She felt that she was useless and that her family despised her for not having a job, though she had sacrificed herself for them. The therapeutic process focused on the development of her personality as a whole (holistic, dynamic approach) [8]. Her “obsessions”, such as painting, meant a lot to her, she always had compulsively driven activities in her life. Blue tones dominated the painting creating a depressive atmosphere, and a hysteric appearance of the whole character, too. The emphasized silhouette of the lips radiated toughness, which attribution could be
generally observed in the patients’ behavior during group therapy sessions (Fig. 5). She refused to soften up her firmness as an organic attribution of her personality and fended off her negative emotions (traumas), though she became really engaded to the art therapy group. As the result of the multifocal therapy she showed significant improvement in her coping mechanisms, her conversive symptoms eventually vanished. At the end of the therapeutic process her psychosomatic symptoms escaped from the focus of her thoughts, so her emotional distress relieved. She had problems with handling conflicts, but eventually she showed a significant progress on that field, too. She went through a therapeutic healing process, which focused on the development and maturation of her personality from immaturity to adulthood (Figs. 6 and 7).
4. Results
The individually customized complex therapeutic system with dynamic approach and integrative therapeutic orientation fits the real needs of the patients. The team succeeded both in stabilization of the psychological state, relapse prevention and the social field enhancing socialization, conversational skills. That means this complex model gave all the patients in the program more chances for social reintegration. The author’s community-like service with different therapeutic modalities proved to be effective in returning patients to productive lives in the community.
The afore-mentioned personal experiences are confirmed by concrete data of the study as follows. The research focused on the efficiency of the complex therapeutic care of the different patient groups separated by the therapeutic modalities.
The number of the patients was 175. The objectives were 1.) Compare the different therapeutic modalities and their efficiencies measured by quantitative
methods and 2.) Differentiate according to the
concrete psychiatric diagnosis, which means to realize the changes measured in the different patient groups.
Fig. 5 Self portrait in blue.
Fig. 6 “I used to be …”.
The psychological tests used in the study are CISS–48 (coping); SCL–90-R (inventory of psychopathological symptoms); Zung (depression) and STAI (anxiety).
The results of the psychological tests according to the therapeutic modalities up to the present are as follows.
(1) Classic static model (pharmacotherapy) versus individual therapy with dynamic approach: The individual therapeutic way confirmed significant reverse tendencies in the grade of somatoform, obsessive-compulsive, mood, anxiety symptoms and in interpersonal hypersensitivity, enmity, trait anxiety, too.
(2) Classic static model versus group therapies (social-, art- and psychotherapy): The patients treated by the methods of the classic model stayed with the emotion-oriented coping, depression and paranoia among these patients remained at higher levels significantly.
The results according to the psychiatric diagnosis are as follows.
(1) The tendency of avoidance-oriented coping decreased significantly in the group of schizophrenics. (2) The tendency of emotion-oriented coping and trait anxiety decreased significantly in the group of patients with mood disorders.
The research program is going to be continued with enlarged method and test batteries.
In the case reports the psychosomatic and depressive symptoms have improved, furthermore the functioning of the patients’ personalities has moved to a more mature direction.
5. Conclusions
In the author’s Mentalhygienic Outpatient Center built up a complex, multifactorial therapic care system, which stands for helping the patients to create and to retain their physical-mental harmony, and to strenghten their social adaptability in order to help their social reintegration. This complex therapeutic
system allows the authors’ team to plan the complex rehabilitation program for the patients, and to ensure, that the patients attend to the programs fitting to their unique needs [9].
According to the author’s basic therapeutic approach it’s the individual himself with his own problems, symptoms, past and present, who is in the focus of the therapy. The therapeutic options are offered within the framework of the author’s multifocal system providing the psychological sense of security. The patients are informed in details and can make decisions with the help of the therapeutic staff. During the therapy the patients proceed step by step and parallel to the state improvement new therapeutic sets at a higher level become available.
All the process of the complex group-centered dynamic therapy proved more effective, than the classic static one [10]. The therapeutic way—with its main stages—could be compared mostly to the maturation and detachment of the frail child. During the care pathways the experiences of the patient have positive significance. The patient can participate in creating and realizing the plan of the treatment as a partner. The patients have positive feelings about the help given and the possibilities offered. The multifocal therapy is appreciated more and more in parallel to the experiences gained, making it easier to establish and strengthen the therapeutic alliance. The author’s team is appreciated by the patients feeling the author’s center a peaceful location of their lives being under cover, where voluntarily and willingly they can participate in the individualized therapy with great success. The leading thought of the author’s therapeutic system is as follows: “When someone helps You, it is not a failure, it means that You are not alone.”
Acknowledgments
thanks the two patients (case reports) for giving their consents to include their histories and drawingsin this publication. Of equal importance are all the clients, who have taught me about the power and value of the complex therapy in personal growth, recovery, and well-being.
References
[1] Kaplan, I. H., and Sadock, B. 1994. Synopsis of Psychiatry. Baltimore: Williams & Wilkins, 197-203. [2] Stetter, F., and Kupper, S. 2002. “Autogenic TRAINING:
a Meta-analysis of Clinical Outcome Studies.” Applied Psychophysiology and Biofeedback 27 (1): 45-98.
[3] Manzoni, G. M., Pagnini, F., Castelnuovo, G., and Molinari, E. 2008. “Relaxation Training for Anxiety: A Ten-years Systematic Review with Meta-analysis.” BMC Psychiatry 8: 41.
[4] Rubin, J. A. 2010. Introduction to Art Therapy: Sources & Resources. New York: Taylor & Francis Group. [5] Cathy, A. M. 2003. Handbook of Art Therapy. New York:
The Guilford Press, A Division of Guilford Publications, 106-111.
[6] Kaplan, I. H., and Sadock, B. 1994. Synopsis of Psychiatry. Baltimore: Williams & Wilkins, 483-485. [7] Erdelyi, K. 2014. “Egyedi Gondozási Utak a Komplex
Ellátórendszer Keretében (Individual Care Pathways in the Complex Care).” Presented at the 8th National Congress of the Association of the Hungarian Psychiatrists, 22nd-25th, Budapest-abstract.
[8] Cuijpers, P., Straten van, A., Donker, T., and Andersson, G. 2011. “Psychological Treatment of Depression: Results of a Series of Meta-analyses.” Nordic Journal of Psychiatry 65: 354-364.
[9] Robert Paul Liberman, M.D. 2010, Felépülés a betegségből. A pszichiátriai rehabilitáció kézikönyve, Oriold és Társai Kiadó, Budapest, Hungary. (Robert Paul Liberman, Recovery from disability: manual of psychiatric rehabilitation, Copyright 2008 American Psychiatric Publishing, Inc.)
Journal of Life Sciences, ISSN 1934-7391, USA
A Comparative Study on Feeding Practice and Nutrition
Status among 6-23 Months Age Children
Taslima Khatun1, Md Shahjahan Matabbar2, Manika Rani Sarker1, Asad-Ud-Daula3 and Asirul Hoque1
1. Faculty of Public Health,Department of Community Nutrition, Bangladesh University of Health Sciences (BUHS), Dhaka-1216,
Bangladesh
2. Nutrition expert, Urban Partnership and Poverty Reduction Project, UNDP, Bangladesh
3. Applied Nutrition and Food Technology, Islamic University, Kustia, Bangladesh
Received: June 12, 2014 / Accepted: August 20, 2014 / Published: August 30, 2014.
Abstract: To investigate the Infant and Young Child Feeding Practice and Nutrition status among 6-23 months age group children in nutrition intervention (national nutrition program) and non-intervention areas.Nutrition intervention has been proposed to reduce the risk of malnutrition. It was a comparative cross-sectional study.A total of 360 households, of which 180 were from the nutrition intervention area each with at least a child aged between 6-23 months were randomly selected. Statistical package for Social Scientists (SPSS/PC+) was used for data entry and analysis. Nutritional status that is weight-for-age, height-for-age and weight-for-height were computed using anthro software. T-test, chi-square and Pearson’s correlation (p < 0.05) were administered to compare the two groups. There was a significant difference between the intervention and non intervention groups in relation to the incidence of initiation of breast feeding, prelacteal and exclusive breast feeding and complementary feeding (p < 0.05). The prevalence of wasting (p = 0.004), stunting (p = 0.015) and underweight (p = 0.003) was observed to be greater for non NNP area compared with the group of NNP area and association was found between those areas. In the study showed that the Infant and Young Child Feeding Practice and Nutritional status are better in nutrition intervention area.
Key words: Under-two children, Nutritional status, wasting, stunting, underweight, nutrition intervention, IYCF and IYCN, Z-score.
1. Introduction
Worldwide, ten and a half million children of age under-five die every year, with 98% of these deaths reported to occur in developing countries [1]. Malnutrition among under-five children is a chronic problem in developing countries like Bangladesh. One fifth of all under-five year old children in the developing world are malnourished and it is associated with more than one-third of all under-five deaths globally [2]. The latest national survey Bangladesh:
Corresponding author: Taslima Khatun, MPhil, research fields: nutrition focused on infant and young child feeding, assessment of diet and nutritional status of different age group (infant, children adolescent, adult and aging), different types of people like farmers, garments worker and ethnic community, nutritional adequacy in different types of diet and consequences of under & over nutrition as well as NCDs. E-mail: [email protected].
Demographic and Health Survey (BDHS) 2011, 41.3% of under-five children were found stunted (15.3% severely stunted) and it also concluded that the prevalence of stunting increases with age [3]. From the same survey, 15.6% children were considered wasted (4% severely wasted) and 36.4% of children were underweight (10.4% severely underweight). Children who are undernourished in the first two years of life and who put on weight rapidly later in childhood and in adolescence are at high risk of chronic diseases related to nutrition [4]. Before/within this period, nutrition interventions are most needed and have the greatest impact on child survival, health and development [5]. Hunger and malnutrition is the one of the heart broken hurdles in the growth and development of the children. Regarding hunger and malnutrition problem it was reported that over 780
D
million people of the world are undernourished and about 13 million under the age of five die each year due to malnutrition and other disease in the world, the great majority of whom in developing countries [6]. Feeding practices have long been recognized as one potentially important determinant of infant malnutrition [7, 8]. Pre-lacteal liquids are harmful to a new born mainly due to two reasons. Firstly, being of poor quality, it increases the risk of introducing early infections to a new born and secondly, as a simple consequence, it reduces the practice of exclusive breastfeeding. Thus, this feeding process can be dangerous to the child and may even results in death [9]. Some studies found that the practice of giving water, honey, sugar water, misry (crystalline sugar), and even cooking oil is universal in rural as well as urban areas [10-12].
It was observed that incidence of diarrhoea was higher among infants given prelacteal liquid compared to the exclusively breast fed infants [13]. Colostrum also contains a high concentration of immunoglobulins, especially immunoglobulin A (IgA) which has a protective role against viral and bacterial pathogens in the gut. The global recommendation was modified and exclusive breastfeeding is now recommended for the first 6 mo of life with the introduction of CF thereafter and continued breastfeeding for the first 2 years [14]. From birth to the age of six months, exclusive breast feeding is recommended, and constitutes appropriate feeding for the infant [15]. Exclusive breast feeding, which means that the baby should be given only breast milk and nothing else, not even water, is virtually non-existent in the country [16]. The composition of breast milk undergoes changes in quality to meet the nutritional and immunological needs of the baby at different stages of child growth [17]. Nutritionally unbalanced complementary food may cause nutrition deficiency disease. Timely initiation of complementary feeding practices among young children helps to promote their Nutritional status minimizing the chances of nutrition deficiency disease [18]. Some workers, however,
believe that food should be introduced even earlier since it has been observed in some instances that growth faltering occurs by 3 months of age [19, 20]. After six months, the frequency of feeding as well as the quality of complementary feeding is significant [21]. Observational studies support the finding that early introduction of solid foods may result in a heavier child [22]. Some researchers have suggested the introduction before 2 to 3 months or later than 6 months, both of which have more risks than benefits [23]. Recent evidences show that the young children of Bangladesh are typically breast-fed for as long as two years or even more [8, 24, 25]. Although this incidence of breast-feeding in Bangladesh is satisfactory, the high rate of child malnutrition signifies the operation of other important factors, such as, inadequate supplementation. Many governments in developing countries implement programs that aim to address nutritional failures in early childhood, raise survival rates, and improve human capital formation [26]. A study conducted at Dhaka medical college hospital were showed that nearly 45.8% were nourished, 1.8% was over nourished and 2.2% were 3rd degree malnourished of under 2 children [27].
2. Materials and Methods
2.1 Study Area
A comparative cross-sectional survey was carried out from January 2011 to June 2012 in sadar pur upazilla of Faridpur district that was an interventional area of Nationaonl Nutrition Proramme (NNP) and subject was carried out from Shoudubi, Mazkandi, Purbokandi, Ramchandro pur, lokharkandi, Noiakandi, Nejgram and Jatrabari villages. This study was also conducted with Goalnando upazilla of Rajbari district that was a non-interventional area and subject was carried out from Aholadipur, Nimtola, Dorpo narayanpur, Rampur, Modhupur, Dudi joypur villages.
2.2 Sampling
According to Bangladesh: Demographic and Health Survey (2011), Implementation Monitoring and Evaluation Department (IMED) of Bangladesh's Ministry of Planning, under 2 children malnutrition (height for age) in Bangladesh, intervention area is 41% and non-intervention area 31% [3]. This assumption and a confidence interval (CI) of 95% were taken into account for sample size determination. Using the statistical formula for comparative studies, a sample size of 350 households was used and multi-stage sampling was done in the selection of households [31].Sadarpur upazilla of Faridpur district that was an interventional area of Nationaonl Nutrition Proramme (NNP) and subject was carried out from eight (8) villages, simple random selection of projects was done. Randomly of the non-intervention area, which had characteristics were similar to the intervention project area. A register of each set of households with children aged 6-23 months was developed and used as the sampling frame. Each household constituted a unit of analysis and had an equal probability of being included in the study. From the sampling frame, 360 households, of which 180 were from each area with at least a child aged between 6-23 months, were randomly selected. In households with more than one
child at this age category, only one child was selected. From the sampling frame, 350 households with children aged 6-23 months and 175 households for each of the study area were systematically selected. This was achieved by first calculating the proportionate sample size for every village. From the list, every household with an even number was selected until the intended sample size was achieved.
2.3 Data Collection
A structured questionnaire was used in the study to collect information on socio demographic and socio-economic characteristics of the households. The socio-economic classification in this study was made according to 2006 Gross National Income (GNI) per capita and using the calculation of World Bank (WB) [32]. (The groups were: low-income $75.41 or less (BDT ≤ 5360), lower middle-income $75.5-$299.58 (BDT 5361-21270), upper middle-income $299.68-$926.25 (BDT 21271-65761) and high-income $926.33 or more (BDT ≥ 65762).
2.4 Dietary Assessment
The dietary energy intake of the study subjects was determined by a 24 h recall method questionnaire and food intake pattern was measured by a specific food frequency questionnaire (FFQ) for 30 days [33, 34]. The nutrientvalue of Bangladeshi food was calculated by using food composition data published by HKI [35].
2.5 Anthropometric
mean measurement was taken and recorded to the nearest 0.1 cm. The body weight was measured using a platform beam scale. The subjects stand still over the center of the platform with body weight evenly distributed between both feet with light indoor clothing. Weight was recorded to the nearest 0.1 kg.
Z-score (Weight-for-Age {WAZ}, Height-for-Age {HAZ}, and Weight-for-Height {WHZ}) were classified by WHO [38].
2.6 Data Analysis
The data were entered and analyzed using Statistical Package for Social Scientists (SPSS) version 16. To ensure that all the information had been correctly entered. Frequencies for non-continuous data and the mean values for continuous data were obtained before carrying out statistical analysis and used in checking for outliers. T-test, chi-square and Pearson’s correlation (p < 0.05) were administered to compare the two groups.
2.7 Ethical Consideration
All ethical issues, which were related to the research involved with human subjects, were followed
according to the guideline of Bangladesh Diabetic Somiti (BADAS) ethical review committee.
3. Results and Discussion
Of the 350 households were enrolled, 175 (50%) were assigned to the intervention group and 175 (50%) to the non intervention group randomly. The subjects were classified by the M ± SD on the basis of NNP and non NNP area. NNP subjects had significantly higher intake of Energy (P ≤ 0.0001), Carbohydrate (p = 0.021) and Fat (p ≤ 0.0001) than non NNP area. No differences in terms of age, monthly income and protein intake were observed between the NNP and non NNP area. The WHZ (p = 0.004), HAZ (p = 0.015), WAZ (p = 0.003) and BAZ (p = 0.011) increased in NNP subjects than non NNP subjects and showed significant association (Table 2). Tests of statistical significance showed that the two groups were similar in the socio-economic and demographic characteristics. The education levels of the population were essentially the same in both the NNP and non-NNP areas. More than half of their father’s had no school education in both the NNP area (64%) and non-NNP area (61.7%). Housewife was found almost
Table 1 Classification of nutritional status using Z-score.
Cut off values Terms of status
Weight for Age Z-Score
< −3.00 WAZ Severe underweight
−3.00 to -2.01 WAZ Moderate underweight
−2.00 to 1.01 WAZ Mild underweight
± 1.00 WAZ Normal
Height for Age Z-Score
< −3.00 HAZ Severe stunting
−3.00 to −2.01 HAZ Moderate stunting
−2.00 to 1.01 HAZ Mild stunting
Weight for height Z-Score
± 1.00 HAZ Normal
< −3.00 WHZ Severe wasting
−3.00 to −2.01 WHZ Moderate wasting
−2.00 to 1.01 WHZ Mild wasting
± 1.00 WHZ Normal
+2.01 to +3.00 WHZ Over-weight
≥3.00 WHZ Obesity
Table 2 Comparing socio demographic and nutritional status between NNP and NON-NNP area of the study respondents.
Variables NNP (n = 175) Non-NNP (n = 175) P value
M ± SD M ± SD
Age 12.5429 ± 6.13 13.2000 ± 6.56532 0.334
Income 10977.14 ± 12020.3 12071.429 ± 8804.17 0.332
Energy intake 413.74 ± 151.94 330.257 ± 104.127 < 0.0001 Carbohydrate intake 38.35 ± 25.011 32.8857 ± 18.701 0.021 Protein intake 7.1600 ± 5.967 6.0629 ± 4.31138 0.050 Fat intake 25.4343 ± 6.948 19.4514 ± 4.42780 < 0.0001
WHZ 0.9026 ± 1.03602 0.9076 ± 1.3269 0.004
HAZ 1.3131 ± 1.451 1.8427 ± 1.7970 0.015
WAZ 1.5218 ± 1.11078 1.8910 ± 1.2932 0.003
BAZ 0.8387 ± 1.14824 1.1895 ± 1.3920 0.011
Results were published as number, t-test was performed and P < 0.05 was level of significance; WHZ = Weight for height Z-score, HAZ = Height for age Z-score, WAZ = Weight for age Z-score, BAZ= BMI for age Z-score.
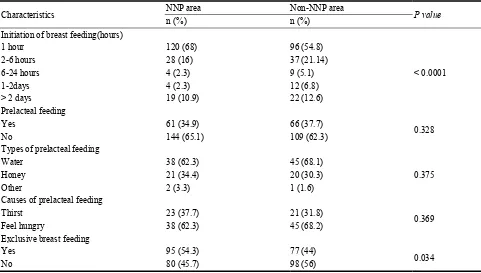
all of their mothers in both the NNP area (96.4%) and non-NNP area (98.3%). The monthly income levels of the respondents were in essence the same both the NNP (78.9%) and non-NNP areas (78.2%) (Table 3). There was a statistical significant difference was found between the groups in relation to their initiation of breast feeding (p ≤ 0.0001), exclusive breast feeding (p = 0.034). Continue breast feeding while interviewing (p = 0.032), breast feeding according their babies demand (p ≤ 0.001). More than half of their mothers initiated breast fed her baby within an hour in both the NNP area (68%) and non-NNP area (54.8%). As regards the prelacteal feeding (p = 0.328), type of prelacteal feeding (p = 0.375), cause of prelacteal feeding (p = 0.369) of their mothers in the study and the control groups, there was no statistical significant difference. Some studies have shown that practices of giving honey or honey with water, sugar water, misry or even oil are universal in the rural communities of Bangladesh [12]. A high prevalence of pre-lacteal liquid is also reported in studies done in India [39]. Another study indicated that the main reason for giving pre-lacteal liquid is no or very little milk secretion immediately after delivery and the mothers could not produce enough milk for the baby [40]. The BDHS data shows that the rate of exclusive breast feeding was 64 % (Table 4) [3]. Significant difference was found between the groups in relation to
Table 3 Socio-demographic characteristics of the study subjects.
Characteristics NNP area (n = 175) Non-NNP area (n = 175) P value
n (%) n (%)
Age of children
6-8month 66 (37.7) 63 (36)
0.710
9-11 month 26 (14.9) 22 (12.6)
12- < 24 month 83 (47.4) 90 (51.4)
Sex of the children
Boys 92 (52.6) 82 (46.9)
0.168
Girls 83 (47.4) 93 (53.1)
Education of the mother
No schooling 81 (46.3) 66 (37.7)
0.087
Primary 83 (47.4) 88 (50.3)
Secondary and higher secondary 11 (6.3) 21 (12) Education of father
No schooling 112 (64) 108 (61.7)
0.342
Primary 49 (28) 51 (29.1)
Secondary and higher secondary 14 (8.0) 16 (9.1) Occupation of mother
House wife 169 (96.6) 172 (98.3)
0.376
Agriculture 3 (1.7) 2 (1.1)
Business 3 (1.7) 1 (0.6)
Monthly income (BDT)
Lower income 28 (16) 25 (14.2) 0.521
Upper middle income 138 (78.9) 137 (78.2)
High income 9 (5.1) 13 (7.4)
Results were expressed as number (%); χ2test was performed and P ≤ 0.05 was level of significance BDT = Bangladeshi taka. Table 4 Breast feeding practice of mother of study population.
Characteristics NNP area Non-NNP area P value
n (%) n (%)
Initiation of breast feeding(hours)
1 hour 120 (68) 96 (54.8)
< 0.0001
2-6 hours 28 (16) 37 (21.14)
6-24 hours 4 (2.3) 9 (5.1)
1-2days 4 (2.3) 12 (6.8)
> 2 days 19 (10.9) 22 (12.6)
Prelacteal feeding
Yes 61 (34.9) 66 (37.7)
0.328
No 144 (65.1) 109 (62.3)
Types of prelacteal feeding
Water 38 (62.3) 45 (68.1)
0.375
Honey 21 (34.4) 20 (30.3)
Other 2 (3.3) 1 (1.6)
Causes of prelacteal feeding
Thirst 23 (37.7) 21 (31.8)
0.369
Feel hungry 38 (62.3) 45 (68.2)
Exclusive breast feeding
Yes 95 (54.3) 77 (44)
0.034
Table 4 continued
Characteristics NNP area Non-NNP area P value
n (%) n (%)
Continue of Breast Feeding
<6 month 72 (41.1) 93 (53.1)
0.032
6 month 95 (54.3) 77 (44)
>6 month 8 (4.6) 5 (2.9)
BF according to babies demand
Yes 139 (79.4) 103 (58.9)
< 0.001
No 36 (20.6) 41 (41.1)
Results were expressed as number (%); χ 2test was performed and P < 0.05 was level of significance Table 5 Information on complementary feeding practice of mothers or caregiver.
Characteristics NNP area (n = 175) Non-NNP area (n = 175) P value
n (%) n (%)
Knowledge on complementary feeding
Yes 124 (70.9) 101 (57.7)
0.001
no 51 (29.1) 74 (42.3)
CF practice
In 6 months 90 (51.4) 68 (38.9)
0.034
Less or over 6 months 85 (48.6) 107 (61.1)
Type of complementary food
Mashed food 139 (79.4) 149 (85.1)
0.023
Chopped 8 (4.6) 25 (14.3)
Both 28 (16) 1 (0.6)
Preparation of complementary food
Family food 87 (49.7) 98 (56)
0.461
Prepared separately 85 (48.6) 75 (42.9)
Both 3 (2.3) 2 (1.1)
Results were expressed as number (%); χ 2test was performed and P < 0.05 was level of significance
respectively. By length for age (LAZ/HAZ), moderate and severe stunted were 16% and 2.8% respectively. In weight for age (WAZ), moderate and severe underweight were 13.71% and 10.28% respectively. BMI for age z score (BMI-Z), moderate and severe malnourished were 12% and 6.28% respectively in NNP area. According to the weight for length (WH-z), moderate and severe wasted were 14.85% and 8.0% respectively. By length for age (LAZ/HAZ), moderate and severe stunted were 16% and 4.55% respectively. In weight for age (WAZ), moderate and severe underweight were 21.7% and 18.9% respectively. BMI for age Z-score (BMI-Z), moderate and severe malnourished were 13.7% and 9.1% respectively in non- NNP area. The prevalence of wasting (p = 0.004), stunting (p = 0.015) and underweight (p = 0.003) was
35% and 18% were stunted, underweight, and wasted; and 16%, 11.5% and 3% were severely-stunted, underweight, and wasted, respectively [42] (Table 6). For the children who received other foods apart from breast milk before completing 6 months of life, the risk of being wasted likely to occur in the non-project area compared to the project area (p = 0.003, OR = 0.442, CI = 0.203-0.959). Who received other foods apart from breast milk too late after completion 6 months of life, the risk of being stunted was 3.9 times more likely to occur in the non-project area compared to the project area (p = 0.038, OR = 3.929, CI = 1.036-14.894). The risk of being underweight children whose too delay to received other foods after completion 6 months of life was 4.8 times more likely to occur in the non-project area compared to the project area (p = 0.012, OR = 4.836, CI = 1.368-17.094). A decrease in prevalence of stunting was observed in both areas as the duration of breastfeeding increased
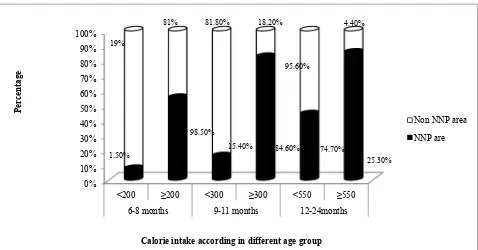
and started complementary food in ideal time (Table 7). According to calorie requirement total children were divided into three age groups in both areas. In the age group of 6-8 months, 9-11 months and 11- < 24 months children had fulfill their calorie requirements about 98.5%, 84.6% and 25.3% respectively in NNP area according to ICMR reference value. On the other hands in the age group of 6-8 months, 9-11 months and 11- < 24 months children had fail to fulfill their calorie requirements about 19.0%, 81.8% and 95.6% respectively in NNP area according to ICMR reference value. The energy intake of three age group such as 6-8 months (P = 0.004) and 9-11 months (P < 0.001) as well as 12- < 24 months (P <0.001) of children had significance difference in both NNP intervention and non-intervention areas. In Faber study, the quality of poor diet was reflected in a poor vitamin A and iron status, and one-fifth of the children showed linear growth retardation [43] (Fig. 1). Nutrition education
Table 6 Nutritional status of the study subjects according to WHO [38] classification.
Anthropometric indicators
Nutritional status
P value NNP area (n = 175) Non-NNP area (n = 175)
n (%) n (%)
WHZ (Wasting)
Normal( ± 1SD) 23 (13.1) 7 (4)
0.004
Mild (-2.00 to 1.01) 120 (68.57) 128 (73.1)
Moderate (-2.01 to -3.00) 23 (13.1) 26 (14.85)
Severe <-3.00 6 (3.4) 14 (8.0)
HAZ (Stunting)
Normal ( ± 1SD) 34 (19.4) 12 (6.8)
0.015 Mild (−2.00 to 1.01) 108 (61.7) 127 (72.57)
Moderate (-2.01 to -3.00) 28 (16.0) 28 (16)
Severe < -3.00 5 (2.8) 8 (4.6)
WAZ (Underweight)
Normal(± 1SD) 11(6.28) 3 (1.7)
0.003 Mild (−2.00 to 1.01) 122 (69.71) 101 (57.7)
Moderate (-2.01 to -3.00) 24 (13.71) 38 (21.7)
Severe < -3.00 18 (10.3) 33 (18.9)
BAZ (Undernourished)
Normal (± 1SD) 14 (8) 14 (8)
0.016
Mild (-2.00to 1.01) 129 (73.7) 121 (69.1)
Moderate (-2.01 to -3.00) 21 (12) 24 (13.7)
Severe < -3.00 11 (6.28) 16 (9.1)

![Table 6 Nutritional status of the study subjects according to WHO [38] classification](https://thumb-ap.123doks.com/thumbv2/123dok/3955145.1898565/27.595.54.546.405.703/table-nutritional-status-study-subjects-according-classification.webp)